Low Oncotype DX Recurrence Score: Do I need radiation?

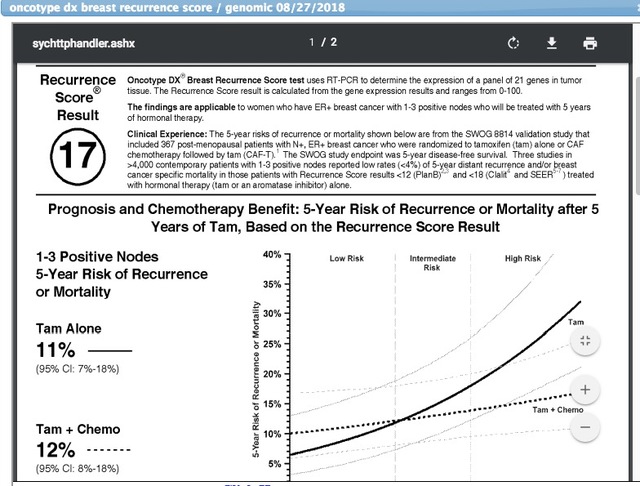
Hi Everyone! My Oncotype DX RS is 17, with an 11% chance of no recurrence with AI alone and a 12% chance of recurrence with AI and chemo. Yes, you read that right. Chemo worsens my recurrence rate. I had 3 lymph nodes removed and with cancer and they also removed the 11 others that had no cancer.
I'm in an area where the docs are, sadly, a little behind the times. I was almost steamrolled into having chemo prior to surgery, and was told repeatedly that I have a high risk of recurrence -- despite the pathology reports that say there was zero cancer except for the one 2.8 cm cancer in my left breast and that found in the three nodes. I'm ER+, PR+, and Her2-. I had a single mastectomy on my left side and am doing reconstruction.
No one--not a single woman or man in my family has ever had breast cancer.
Experiences, suggestions? I'm getting a second opinion from a different rad onc this Friday. I'm looking forward to hearing what he has to say.
Cheers!
Comments
-
It seems there may be more concern with 3 nodes involved. Just guessing. The percentage of recurrence refers within the first 5 years. Sure doesn't hurt to get a second opinion, but radiation seems to be the standard. Someone will chime in shortly. We have a contributing radiologist on this site. Will check to see his thread. Hugs and hang in there
 0
0 -
Go to Just Diagnosed and scroll back to djmammo's post. You can send him a private message
0 -
I had an Oncotype score of 11 and had radiation. 33 treatments. One micromet in my SN. You had 3 nodes with cancer. 17 isn’t high but it’s not that low either. I would have the radiation. Definitely get a second opinion though if it makes you feel better.
Diane
0 -
I believe the recurrence scores are based on tamoxifen use not AI drugs. It has been 7 years since I had my oncodx test so maybe they have updated with AI use.
0 -
I was post menopausal (62) and my recurrence rate was based on lumpectomy + radiation +aromatase inhibitors
0 -
JoE777, was it from the oncodx report?
0 -
Meow13–I might be confused about what an AI is. Yes, the Oncotype DX is based on tamoxifen, but Arimidex (anastrozole) is indicated as a substitute that gives better results for postmenopausal women.
Thanks for chiming in! I'm going to talk to my new rad Inc about this issue.
0 -
Tajmari Did your doctor tell you that you were stage 1B? I only ask because my understanding was that the tumor needed to be less than 2 cm and the nodes could only have micromets up to 2mm to have a stage 1B diagnosis. Maybe this is due to the new staging guidelines? Best wishes!
0 -
With cancer found in the lymph nodes, I'd definitely have the radiation. I had one positive node, and am glad I was able to get radiation to that area. Always your choice though! It's hard I think when they give us these options, because no one can see the future and yet we always try!
0 -
Yes, my oncologist told me I was 1B. However, my new radiation oncologist (yes, I'm going with the new guy) told me that they (the entire medical community) has recently switched to a new rating system, so I'm back to a 2B. It doesn't make sense. It is the same tumor. ;-) Anyhow, I qualified for the Oncotype DX test, thank god! The test showed I would be worse off with chemo than without.
My new radiation oncologist is great. He talked to me for about 2 hours even though the nurses told me they are so busy at his office that they are running the machines three hours late every night.
Based on his advice, I'm going to do radiation as it will reduce my chances of the cancer recurring. But, since my cancer was on the left side, there is actually a rather serious danger of heart damage due to the radiation. My new doc is the kind that uses high tech scanning and computerized targeting and we are going to go over it carefully and he will meet with me before we start.
I won't start radiation for another month because I need to finish my breast reconstruction. Fortunately, my rad onc is friends with my plastic surgeon, and they had a confab about me.
It's all good.
Cheers!
0 -
Thanks, GB! There are downsides to radiation, and I'm glad my doc explained everything to me in detail. His office even had a short film that shows how the machines work and what to expect.
Cheers!
0 -
Meow, yes
0 -
Hi! letsgogolf et al- Here's research from 2016 on close to 7,000 patients that shows excellent results without chemo for patients with 1-3 poistive nodes and/or some micromets:
http://www.genomichealth.com/en-US/Advocacy/New_Node_Positive_DataOncotype DX Accurately Predicts Clinical Outcomes in Patients with Node-Positive Breast Cancer
At the most recent 2016 European Society for Medical Oncology (ESMO) Congress, results were shared from two studies involving the SEER (Surveillance, Epidemiology and End Results) program of the National Cancer Institute (NCI) and the Clalit Health Services, the largest health care services provider in Israel, showing the clinical utility of Oncotype DX in predicting breast cancer outcomes in patients with early-stage, node-positive disease.
The SEER study, recently published in Nature Partner Journals Breast Cancer, demonstrated that the Oncotype DX® Breast Recurrence Score™ (RS) test accurately predicted prospective patient outcomes, including over 6,700 patients with 1 to 3 node-positive breast cancer.
The SEER results presented at ESMO include additional data and follow-up for patients, linking the Registry data of breast cancer cases from 2004 to 2013 to Oncotype DX RS results. In the 3,919 node-positive patients with an RS less than 18, five-year breast cancer-specific survival was excellent with a survival rate of over 97 percent in patients with micrometastases and one and two positive nodes.
Additionally, results from the Clalit retrospective study examined the records of more than 700 patients tested with Oncotype DX. A vast majority (92.9 percent) of patients with a RS less than 18 with either micrometastases or one to three positive lymph nodes who were treated with hormonal therapy alone had very good outcomes. They had a low rate of distant recurrence (3.2 percent) and excellent breast cancer survival (> 99 percent) at five years.
"Just as we have learned in node-negative disease, it is now increasingly evident that women with one to three positive nodes and lower scores do extremely well without chemotherapy," said Kathy S. Albain, MD, FACP, FASCO, Professor of Medicine, Loyola University Chicago, Cardinal Bernardin Cancer Center, Maywood, Illinois. "These data, along with previously published results, provide extremely strong evidence to justify use of Oncotype DX in 1-3 node-positive disease. If the patient's tumor biology is that of a low Recurrence Score, chemotherapy simply does not add benefit, and its risks and costs can be avoided."
Cheers! -- Taj
0 -
Tajmari That is good news for those of us with micromets or just a few positive nodes. My Oncotype score also showed a worse outcome prediction for me if I had done chemo. Many people automatically think that more treatment is better but that is not always the case, especially in Luminal A cancer.
0 -
Letsgogirl: Thanks! You're the first person I've heard of whose OncotypeDX showed a worse outcome with chemo than without. My rad onc shook his head in disbelief.
Not sure if this will work, but here's a link to a screenshot of my Oncotype DX report:
 ?dl=0
?dl=0Cheers! - Taj
0 -
In patients with IDC, OncotypeDX is used to determine the advisability of adding chemo, not radiation, to endocrine therapy. In IDC patients who elect lumpectomy rather than mastectomy, radiation is a given. The confusion here may stem from the fact that in patients with DCIS, the score is used to determine which lumpectomy patients can skip radiation.
0 -
ChiSandy, Thanks! Yes, my RO told me that Oncotype DX assumes "standard" care. So that means for me, with IDC and a mastectomy (not radical, but still a mastectomy), I should also have radiation, which I agreed to do per his explanation of risks/benefits. With radiation, most people actually don't benefit, he said (67%), but there is no similar test such as Oncotype DX that has been tested for radiation. Or, at least, that's what I gathered. It's very confusing. But, I'm in heaven knowing that I can skip chemo.
I finally figured out how to upload a screenshot. @Meow13 - Note that the results say in small print that either tamoxifen or an AI can be taken. Here's my Oncotype DX score:
Cheers! - Taj
0 -
My Oncotype score was a 3 and the risk of recurrence or death is 4% without chemo and 7% with chemo. I imagine that is due to the damage chemo can do to our bodies.
0 -
Tamoxifen seems to be equally as effective for er+ pr+ cancers. Not the case for er+ pr-, AI drugs more effective.
0 -
@letsgogolf - Great numbers! Yes, I believe that my higher (12%) score WITH chemo than without (11%) stems form the damage/death that chemo can do. There's a differene, my RO said, between OVERALL rates of recurrence/death and CANCER-SPECIFIC rates. As I understand it, the Ocotype DX score is based on overall rates, which is the best comparison because it takes into account the deaths/recurrences that occur as a result of chemo or rads.
Best! -- Taj0 -
Tajmari-Thank you for this clarification. I was also told that there is nothing like the oncotest for deciding on the benefits of radiation. Instead I was told itcomes down to risk verses benefit. If surgery, chemo, and tamoxifen reduces your chance of reoccurrence to a very small number you may decide that radiation risks are higher than the benefit for example. Also age is a facto, at 45 I was advised to do rads but if I had been inmy 60s they would have said it's not necessary.
0



