i have more delays...is it bad or i am overreacting
Comments
-
thank you MinusTwo.
I would like to fill out My Profile after pathology report after my surgery yesterday....it would be more accurate i think.
0 -
You can put what you know now and add to it or change it any time.
0 -
I added now. but it does not show up?
0 -
Radiation usually starts when you have healed enough, about three or four weeks? I had to have another unrelated surgery after lumpectomy (and re-excision), and the breast surgeon and radiologist were insistent that I wait no more than 12 weeks from the re-excision to start radiation.
0 -
My radiology oncologist scheduled me to start rads four weeks post-op. She wanted everything nicely healed before the rads.
0 -
In 'My profile' you have to check a box to make the information public for it to show up.
0 -
Hello, I don't know yet result of my pathology report ...after surgery.
But i had very weird situation today(it seems weird to me), so please let me know what you think about it.
Last week i wrote on hospital portal a message to doctor office: "I know that doctor is away and my post op appointment is on 1/6, but is any way i can find out a result of pathology report earlier?" My surgery was 12/19...
I got a response from nurse Megan: "You can give me a call Monday or Tuesday to see if the results are in"
I called monday and was told that Megan is sick but they checked for me and said results are not in yet.
I did not call tuesday.
Today at 9:30 a.m. i got voice mail from Megan, she was saying : please call office when you hear this message, i have some good news for you.
I called back around 12p.m.( i was working and missed her call and only noticed voice mail later), i asked her...and office secretary(or whoever) went somewhere, came back and said: she is waiting for doctor call...and she would call you back after that.
in 2 hours...no one called, i called back and spoke to secretary again. I told here that Megan left me a message at 9:30 a.m. and i am anxious now ....want to talk to her. Secretary said: she is waiting for doctor email, he is out of country, you know, she will call you back after.
No one called today still....
I don't even know what to think now. I mean : i can understand that she may be need his clearance to let ppl know pathology report details, but why on earth she called me at 9:30 a.m. ...to give me good news, as she said, and then ....just no news at all.
Please let me know what you think of this situation. thank you
0 -
o...no one has anything to say ....i guess to me.
0 -
sorry no thoughts. I guess just keep calling until you get this nurse.
0 -
It's the first day back after a holiday and the doctor is traveling out of the country - I'd be shocked if there WASN'T a communications breakdown. I had an incident once where I was in the hospital all hooked up to IVs and ready for surgery, waiting. And waiting. And waiting. And the nurses and anesthesiology team were freaking out because the surgeon was a no-show with no word on the delay. Finally, after a couple of hours, we found out he'd had a family emergency out of town, and he'd left a message with his office - but mine was an early morning surgery a few hours before any office staff had arrived, so the hospital didn't get the message. I was cranky (and hungry!) but it didn't adversely affect my health. Everyone involved is human and these things happen.
0 -
Ditto what AliceBastable said. You had the misfortune of having surgery just before Christmas and New Year's, and with offices and labs closed for several days during this period and with fewer and inconsistent staffing, there are bound to be delays and communication problems.
The good news is that the nurse said she had good news for you, so while you are still waiting, you have every reason to be hopeful that the pathology results are good.
0 -
thank you, dear all.
as we all say here a lot: waiting is the worst.
i was ok emotionally...but it does not take much to throw me off the balance.
thank you for support...i will try to stay calm.
now i am thinking that good news just meant: report is ready....but this is me being afraid of think optimistically that
good news...meant more than that.i will let you all know as soon as i find out
0 -
You have to heal from surgery before you can start rads. Your BS will let you know when you're cleared to start treatment. I think a month is typical.
0 -
I strongly believe that "good news" meant a good pathology report!
0 -
MikaMika, thank you!
I will try to think that during this weekend, because no one called me...I called back today and just did not ask for nurse but said: i would like to find out result of my pathology report, the secretary looked up my chart and said: it is here...but i have to ask clinical team to call you back with details...and guess what: no calls(which i was not surprised), not sure if nurse is part of clinical team...
so i have to live thru this weekend, and my doc appointment on monday 10:30.
0 -
marinochka,
how are you doing?
0 -
Hello, thank you for asking MikaMika
I got my pathology report, there are good news and one a little not good(but not unexpected).
good news: nothing invasive was found. it is still the same : stage 0, DCIS, grade 2
also good news: in the area when biopsy showed DCIS ...it is all clean now, it was removed with calcification during biopsy.
also good news: it is ER+ 100%(i was scared of triple negative, my biopsy showed ER+ but no %, so i was concerned if it is very small %, and in this case it is treated as triple negative)
Not so good news: on one side 0.5mm from "main area of lumpectomy" tiny DCIS. which makes on this side margin 1.5mm not 2mm, as all other sides, and this is what goal was.
Doctor said that he would recommend to leave it like that but it is my decision , i insistent on re incision and making on that side bigger margin.
He said if all tissue will be clean what he now is planning to remove, i might not need radiation. this we will have to see.
Re incision is on 1/16.
I was confused first ...and what bothers me : if this is another DCIS ...do we get all of them now which are there ...
Please comment dear all.
thank you
0 -
marinochka,
Congrats with the mostly good news! Did you celebrate?
") A cake? An ice cream? 0
A cake? An ice cream? 0 -
MikaMika, no, not yet...it is ok, i hope to have more reasons to celebrate...
0 -
Just suggesting--
I think there is a pretty active DCIS discussion board in this community too; they probably have a lot of insight for you. Have you tried posting some of your questions there, too?
Claire in AZ
0 -
hello, had my re incision today to get bigger clear margin on one medium side.
It was quick and I feel fine.
I was told that because it it second time, more chances of bleeding and infection, so I have to be careful ... and also to wear a bra 24 hours till I see my doctor. It needs pressure to avoid bleeding.
Pain, I was told, also could be more severe , but not yet, it is minor now.
I asked before that surgery to have dcis oncotype test( in email on a portal)When surgeon came in to greet me before surgery, he said: oncotype test does not show anything ... we use a different one, we will talk about it on 1/31
My post op appointment 1/31.
0 -
marinochka,
How are you doing?
0 -
Hi, MikaMika
I had a post op appointment and tissue which was removed during my re incision is clean. Nothing was found there.
And i have 1 cm margins now. I will have a appointment to see RO next week and will discuss rads.
I feel optimistic now. thank you for asking!
0 -
Great news! I am so happy about you!
0 -
My update from today appointment with RO:
He was not insisting to leaning to either : do radiation or not to do radiation.
He said that to do nothing now would not be a good decision. But it seems to me that he wants me to choose between radiation or hormonal treatment.
He does not think that i need both. But I will see MO on 2/19, so he wants me to talk to MO ...and decide. Or I can try to take Tamoxifen for 2 weeks and see if i totally hate it and give him a call. Meaning I would stop then Tamoxifen and do radiation instead.
He said that i have 3 months from a surgery to do radiation(even more, but he would say not to exceed 3 months).
I asked him about proton therapy. They have it available, but he said it would not work for me. My understanding is that they don't do it for the whole breast, and i would need radiation for the whole breast, he said for 4 weeks.
With radiation next 12 years recurrence risk, he said, 2-3%. Without radiation : 12%. But i already looked up their nomogram, and if i do nothing it is 12%.
If i do hormonal therapy and no radiation it is 5% -5 years, and 7%-10 years. I said it to him, and he agreed with information WHICH I TOLD HIM.
So how come you are saying to me 12%...It is frustrating.
He said that because of my UV sensitivity I will be at risk for skin complications, but he did not have cases like that before.
He also lightly said : if it comes back we will radiate it then... But i said that it could be invasive then. And he said : yes, in 50% of cases it is invasive.
I left the office with more inclination not to have it than to have it...but I am not sure ...tortured again with doubts.
Anyway i have time till 2/19 and will discuss with MO further.
Any comments would be greatly appreciated.
0 -
I think the point your RO is making is that with such a small grade 2 DCIS, doing both radiation and endocrine therapy would be over-treatment. So he's suggesting you do one or the other.
With a very small area of DCIS, I don't know why whole breast radiation would be necessary, but then I don't know much about radiation. To your PM, it's true that whole breast rads would treat the entire breast but if there is no DCIS or cancer anywhere else in the breast, that's a useless benefit. Rads will reduce your risk of recurrence from your current diagnosis, but it will do nothing to stop a new primary from developing in 3 years or 10 years.
Endocrine therapy, either Tamoxifen or an AI, will reduce your recurrence risk from this diagnosis (by about 45%) and will reduce your risk of a new primary in either breast.
Just my opinion, but I believe the MSK nomogram is over-estimating your recurrence risk, both because it doesn't account for the extremely small size of your area of DCIS (much smaller than average) and because it doesn't account for your wider-than-average margins (thanks to the re-excision). The nomogram also may be over-estimating the benefit of rads - most studies (and there have been lots of them) suggest a 50% risk reduction from rads, although one recent study did suggest a 70% reduction in risk. Or did the RO mean that with rads and hormone therapy combined, your risk would be 2%-3%? That would make sense (assuming the 12% risk after surgery alone is correct). But with rads alone, a 12% risk could be reduced to 3.5% at best, and more likely (considering all the studies) 4%-5%. That would mean just a 1% -2% difference between the risk reduction from rads alone vs. the risk reduction from endocrine therapy alone.
As for your risk without any further treatment, based on the Van Nuys index, you score a 5 (almost a 4, given your age), which is the best possible result and suggests a 12 year recurrence risk of 6% or less, 1/2 of what the MSK nomogram is telling you.
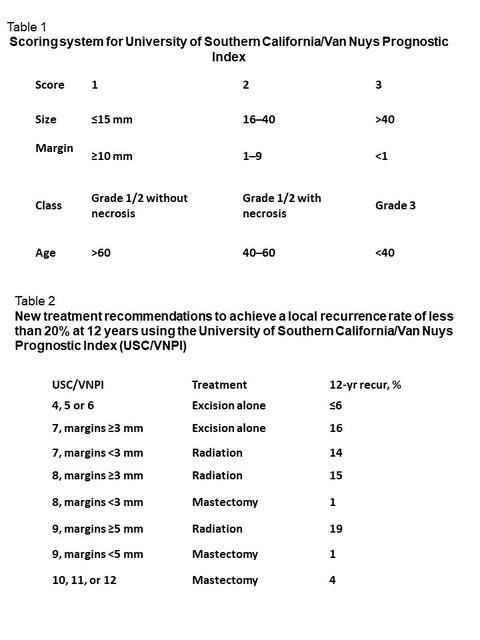
Given the unusually small size of your DCIS and the wide margins, I lean towards the Van Nuys Index as being more accurate. Or maybe the best guess is to split the difference and estimate an 8% recurrence risk with no other treatment. With radiation alone, this could be reduced to 2.5%-3.5%. With endocrine therapy alone, this could be reduced to 4.5%.And then there is your risk to develop a new primary, which is higher than your risk from this diagnosis, and which only endocrine therapy can reduce. Which isn't to say that endocrine therapy is a better option for you, but is just one more consideration
Lots of questions for your MO, I think.
0 -
thank you Beesie for your reply.
Which questions you would recommend to ask MO?
and also how it is decided between Tamoxifen or an AI.
And may be i am ahead of myself but I know a few women who after a year after breast cancer diagnosis(in their 60th) ...still have ovaries removal surgeries.
Not sure about hysterectomy.
thank you
0 -
Just popping into say, if you choose whole breast radiation, they give you a life time dose and that area would not be able to be radiated again. I think that's why the RO said IF it comes back we will radiate then.
I can't see if you are pre or post menopausal? They can do a blood test for it if you are unsure. Usually Tamoxifen is given to pre menopausal women. It can also be prescribed to post-menopausal women who cannot tolerate the AI drugs. Mostly post menopausal patients are given the AI. There are some pre menopausal patients taking an AI too, but they are also doing some sort of ovarian suppression, or removal. All of the meds are options either way.
Hope that helps, a little
0 -
"Just popping into say, if you choose whole breast radiation, they give you a life time dose and that area would not be able to be radiated again"
This was not the case for me. I specifically asked my RO about it and was told that I would not be getting even near my lifetime dose. I asked what would happen in case of recurrence and they said that they are seeing cases of women having second lumpectomies with second radiation depending on the location/nature of the new tumor.
0 -
Interesting Salamandra. I had always heard rads to any specific area was once done just like ctm. Yes, I could have rads on the other breast, but not the one that was previously zapped.
0




