Should I sue?

-Started chemotherapy on 4/2021
-Finished 7/2021. MRI of chest showed everything is clear and was told by former oncologist that I am in remission.
-Had a fall on August 2021: MRI showed lesions on my hips and a lump the size of an acorn on my sacrum. Bone biopsy results showed it is adenocarcinoma metatastasis with mammary origin.
Very angry at former oncologist. Can I sue her?
Comments
-
What grounds do you feel you have for a law suit
0 -
I agree with exbrnxgrl, what grounds do you feel you have to file a lawsuit? Did your MO's treatment not follow the accepted guidelines?
0 -
Would the issue not be with whoever read the MRI? I would be wondering how come you never had at least a CT scan and a bone scan as part of your treatment.
Was a chest MRI the only imagine you had before your MBC diagnosed?
0 -
A malpractice attorney will be in the best position to evaluate the potential success of a lawsuit.
A good malpractice attorney will be very upfront with you about the potential financial, emotional and logistical impacts of a potential lawsuit.
If a malpractice attorney really believes in the likely success of a case, they will probably work on contingency, where you do not pay unless you win. If an attorney is unwilling to do that, it is probably a sign that they don't believe your case will be successful or win an amount of money that will compensate their expenses. At that point, if a person continues, they are generally suing on principle or in an attempt to resolve feelings. This generally is bad for their quality of life unless money is really not an object for them and they are sufficiently emotionally supported/distant enough to be able to proceed without having it take over their life.
A lawsuit against the doctor won't resolve feelings of anger or fear about cancer. Therapies like chemotherapy do not work 100% of the time, and it doesn't mean the doctor did anything wrong or that you did anything wrong. Sometimes it's just luck.
When someone is considering suing anybody over anything, I usually think the best step is to consult both a lawyer and therapist. Otherwise people try to use the law as therapy and it's bad for everybody. In consultation with experts (lawyers & therapists) people can make a better decision about what path will be the most practical and effective for them going forward. If they do decide to go forward with a lawsuit, a therapist can be just as important for providing ongoing support and processing. They may also provide alternate suggestions for things you can do to help you feel like you've taken action and communicated your feelings that are not as costly or destructive as a lawsuit. These might be things like writing to the doctor, their practice, or possibly even their board.
Yes, this will have an initial outlay of costs. But generally it's an ounce of prevention for a pound of cure.
I'm so sorry to hear about your progression, and I wish you better news from here on in.
0 -
If your medical team followed standards of care, there may be no legal basis for a malpractice judgment. I'm not sure if you're most concerned about the chemo or treatment used (you say you had "Other" chemo) or about not having the scans that found the metastasis sooner. Having the scans sooner would not have kept it from happening. Also, having a bunch of scans to look for MBC is NOT a care standard. They don't look unless you have symptoms.
As Salamandra said, sometimes it's just luck. Random shitty luck. I'm very sorry.
0 -
lotus,
I am no expert and not familiar with the particulars of your situation but from what you’ve noted it appears as if standard of care was followed. If it’s any comfort, I was staged IIB after my bmx. Long story but about six weeks later my bone met was found on an unrelated PET scan. No one to sue, no one to blame. It was just a completely unexpected finding. These situations are not common but do occasionally happen. I know it was probably quite a shock but your mets likely started growing before your tx not since your tx without any reason to suspect they were there.
Sunnidays,
Scans are not standard of care for stage I patients. An MRI of the chest could not have visualized mets on the hips or sacrum.
0 -
exbrmxgrl, you are correct,I remember the oncologist the first time explaining why they only scan if there are symptoms.
It never really occurred to me before but oncology must be a very difficult career and perhaps my oncologist's slightly brisk demeanor is a protective measure for herself. I know I could not do the job I would be overwhelmed, imagine having to tell a young parent that there is nothing else they can do for them.
0 -
Anger can be a normal response. Cancer comes back sometimes. And sometimes it doesn't come back. None of my doctors missed anything. My anger is directed toward the disease and what it has done to my life and my husband.
A lawsuit is a serious thing, but should be considered, in my opinion, only if your medical care and treatment were severely botched.
0 -
When you were diagnosed, before they decided on your treatment, did your doctors order any image to confirm if there was metastatic disease?
I believe you only have grounds to sue for the real clearly attributable and catastrophic mistakes, like they didn't follow the standards of care, or you were supposed to have breast cancer surgery and they removed a kidney instead.
Wise words from Salamandra about lawyers and therapy. Had never thought of that.
Very sorry you got this news. I extend all my sympathy. That is a very hard pill to swallow. Sending you hugs.
0 -
LaughingGull, "before they decided on your treatment, did your doctors order any image to confirm if there was metastatic disease?" This would not be typical in the US unless your symptoms and early pathology suggested a spread of disease from the beginning.
0 -
As I said in my other reply, unless they didn't follow normal standards of care, then I don't see what the grounds could be. Cancer can & does come back, and sometimes very quickly.
Post treatment scans in the absence of symptoms are not recommended by any of the clinical guidelines that I've read.
The only thing that made my eyebrow go up is the word remission. It's rarely used in solid tumor cancers. It's a hematological cancer term (leukemia, lymphoma etc). For solid tumors they tend to say No Evidence of Disease...because that's all we have, no evidence. Doesn't mean it's not there.
Scans cannot pick up individual cells and cancer metastases can grow very quickly. Many of us dealing with metastatic disease have had changes in scans taken 8 weeks apart. I had one scan repeated at 4 weeks for clinical trial entry & I had growth in mets during those 4 weeks.
I think in early stage cancer growth is a lot slower; but metastatic disease can be like an out of control forest fire.
I'm sorry you have this diagnosis. It really sucks but there are some very effective treatments to keep it at bay for a while.
0 -
laughing gull,
As has been stated several times, scans are not standard of care for early stage disease.
0 -
sunnidays, Many years ago, I worked in a hospital as a unit secretary (long before everything was computerized, we were the ones who kept all the orders and vitals results organized). I was on a surgical floor, but there was an oncologist who would come to see his patients who'd had a cancer-related surgery. Especially with the younger patients, he would stay for hours, holding their hand while they slept, or talking to them about anything and everything if they were awake. The nurses and other floor staff would do anything for him to make his life easier, as he made his patients' lives as comfortable as possible. If any other doctor had asked, for instance, to get them coffee, we'd have told them FU. With this one, he'd never ask for anything for himself, but we'd bring him coffee or ask if he wanted things because we all loved him and what he did for his patients. And if one of his patients died, he mourned with and comforted the family. I'll never forget him, and I only worked there about a year.
0 -
Standing to sue has three parts (in the United States):
1) the defendant caused the plaintiff to suffer a direct and significant injury (injury-in-fact)
2) the harm is traceable to the alleged unlawful action of the defendant (causation)
3) that harm can be remedied through legal action (redressability)
The problem you have is with 2). Were your doctors negligent? Can your mets be traceable to their actions or non-actions? As others have said, if your doctors followed standard of care, they may not be deemed negligent.
0 -
I have nothing to add that hasn't already been said about a lawsuit. LotusNoirAmethyst, so sorry to hear of your Stage 4 diagnosis.
Moth--I have to say, this is one of the most profound statements I have read in a while... "For solid tumors they tend to say No Evidence of Disease...because that's all we have, no evidence. Doesn't mean it's not there."
0 -
Lotus, I'm so sorry you have this dx.
I , too was stage 1 , node negative and completed surgery, Chemo and radiation plus 6-7 years on femara. Never had a pet scan as I was stage 1 (had mri and of course , mammograms ). When I had symptoms (laryngitis for months) my GP insisted it was a virus and refused to order a scan . Cancer center (was seeing a "wellness onc PA" bc I had very low risk of recurrence per Seattle cancer care alliance ) refused to scan me , mammograms were beautifully clear. I offfered to pay for scan out of pocket but was refused. I finally saw an ENT who ordered a CT, led to biopsy and body scan and here I am . I was told over and over that stage I = no scans without symptoms , standard of care. But, even with symptoms it took months for me to get a scan.
It's criminal in my opinion l but I don't think would be considered negligent as it is within "Standard of Care" .
0 -
Lotus, I am sorry that you are dealing with this.
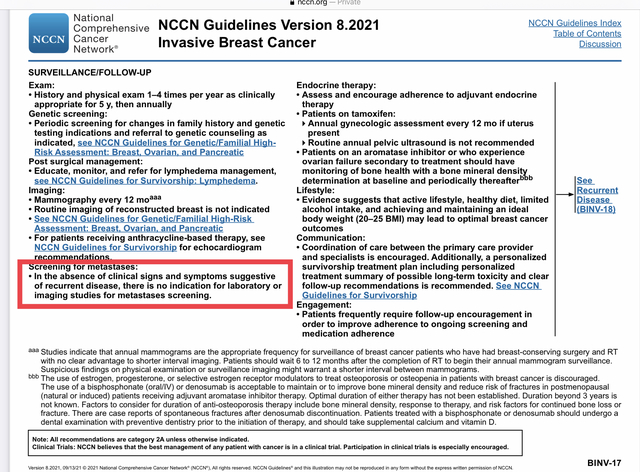
To the previous comments, here are the current NCCN Treatment guidelines for the workup at time of diagnosis, and for follow-up screening: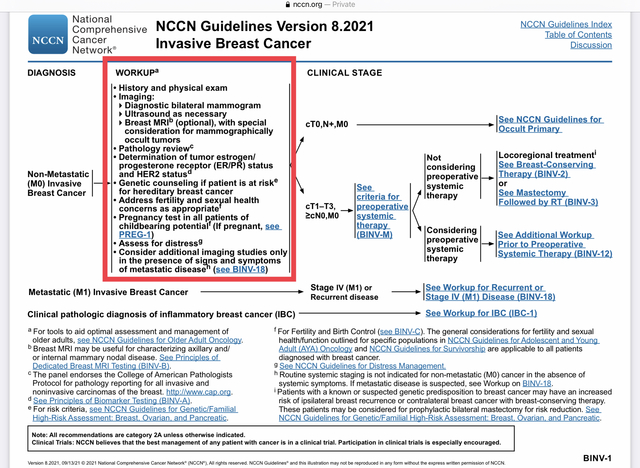
moth, while I haven't often heard the term "remission" used for breast cancer, I have sometimes heard it used. It effectively means the same thing as NED in tha it refers to the signs and symptoms of the cancer but not the cancer itself.- "Remission: Disappearance of the signs and symptoms of cancer or other disease. A remission can be temporary or permanent." https://www.medicinenet.com/remission/definition.htm
- "Complete remission: The disappearance of all signs of cancer in response to treatment. This does not always mean the cancer has been cured. Also called complete response." https://www.cancer.gov/publications/dictionaries/cancer-terms/def/complete-remission
0 -
Lotus - lots & lots of us have had treatment only to have either a "local recurrence" or even "mets". It's my understanding that no one is EVER cured. You can be in remission or have "no evidence of disease". Agree with all the above comments. Standard of care is definitive. Of course you're angry, but it doesn't sound like the doc said "you're cured". Personally I would turn my anger towards making the best progress I could with whats coming next. If you don't trust that doc anymore, find another one.
0 -
Aprilgirl,
My situation is not exactly like yours, but my met was found by accident before I even started tx for what was thought to be a stage IIB tumor. I don’t really think it’s criminal because situations like ours are simply rare, unlucky occurrences. PET scans are prohibitively expensive and expose you to a lot of radiation. Stinks for the rare birds like us but I still support the standard of care.
0 -
exbrnxgrl, I am still not over the fact that I had to fight so hard to get doctors to listen to me about my serious concerns and symptoms . I have great insurance and offered to pay out of pocket. It sucks and it was so frustrating. Luckily, I am doing well on tx - two years now. I chose to focus on this and feel fortunate that I feel good right now ! Criminal might be the wrong word but ignoring patients pleas should not be "standard"
0 -
just to add to this discussion, the reason they do not recommend the scans is that there is no proof that finding mets earlier is associated with longer survival
& the scans carry their own risk - exposure to radiation or contrast agents etc
So they wait for symptoms of metastatic recurrence & use physical exam & patient reporting. That is why pts should be closely followed by a physician who is aware of their medical history. In a pt who has had cancer before & has a new otherwise unexplained symptom which persist, metastatic disease should be on the differential diagnosis list.
aprilgirl, re recurrence in distant lymph nodes only - I've seen oncologists discuss whether that should be treated as 3C ie. with curative intent. I know someone online with a lymph only met who is NED 5 yrs now.
0 -
@Moth, I agree. I go to Seattle Cancer Care Alliance andam still surprised at how hard I had to push to get scans . I brought an article from 2020 about distant nodal Mets and the restaging and my onc doesn't agree but considers it somewhat like bone only mets. I had some cancer in tissue in the hilar area . I am lucky I have had a great response so far. I do have an ATM mutation that was discovered in 2018.
0 -
April,
I’m sorry you were frustrated by the fight. It seems as if different facilities and doctors follow various criteria for who gets scans or not. My mbc dx came so quickly after my bmx that it’s a bit of a jumble now but once my mbc was confirmed, my mo never hesitated to order scans if I was experiencing pain for more than two weeks. That mo has since moved back to her home country (the nerve! 😉) and I haven’t had any out of the ordinary pains recently with my new mo. Take care
0 -
lotus,
Being upset with your oncologist is not a Breach of Standard Care for a medical malpractice suit, and medical malpractice is HARD to prove and varies in each state. If something got missed, it would be on a provider, such as a radiologist who misread a scan, a pathologist who had incorrect pathology, or a provider who incorrectly prescribed treatment. In any event, that event must cause you harm or injury.
Getting a stage IV dx is not a Breach of Standard Care if doctors provide the standard of care, which could be different in every state and facility. While having to push for scans baffles me, it happens often, and it is not the standard of care in the NCCN guidelines to scan for stage IV without symptoms. Sometimes the solution is to switch providers to get the RIGHT treatment.
Furthermore, if a suit were a consideration, you would not want to post about it publicly, and blogs and social media would be better left with words unsaid.
I am sorry this happened to you. It must be a tremendous challenge. I hope to read that you get good results with your treatments.
0





