Minimally Hormone Receptive

Hi! My cancer is technically ER+/PR+ however the hormone levels are minimal— 2% and 1% respectively. The MO wants to treat the cancer as if it were triple negative— with chemo. I am BRCA1 positive and small tumor. I had a BMX, the nodes came back clean and I was classified as Stage IA. Oncotype was not done but she's willing to submit it but she's confident the score will come back high. The MO wants to give me chemotherapy as a way to make sure any potential outlying cancer cells are killed. She said hormone therapy would do me little good compared to the side effects.Of course, it's my choice as to what to do.
I'm wondering how I should classify myself —am I really ER+ positive, a triple negative or something in between? Has anyone else been in this position? What treatment options were recommended?
Thanks!
Comments
-
I am PR- and 3% ER+. My MO considers anything over 1% positive. I had chemo and rads, grade 3, 1/5 lymph nodes, BCRA negative. Currently, on exemestane (aromasin). I didn't have an oncotype done.
0 -
Since you are positive for BCRA, I wonder if you can get that brand new FDA approved drug. They say side effects are minimal. I think it is used for prevention, cost $13,000 a month might be a problem for insurance.
http://www.omaha.com/livewellnebraska/fda-approves...
0 -
Thanks BravePoint for sharing. My MO thinks hormone treatment is better received if levels are 10%. it sounds like there is varying guidance.Based on your comment, I think I will go get a second opinion regarding treatment options.
Meow, that’s good to know! The article mentioned it’s for advanced cancer so with me being stage 1A I wonder if I will be considered a good candidate. But it can’t hurt to ask!
0 -
Hi! I wanted to provide an update. This week I received a second opinion and they recommended chemotherapy as well. I also received my Onco score and it was 48. I would encourage anyoone that has low positivity to get their Onco score to see if chemotherapy will be more beneficial than hormone treatment.
There's a limited time between surgery and when you can start treatment so I'll start treatment this Thursday.
0 -
So glad you got good advice and have a plan. Best wishes to you.
0 -
FaithWalker - just chiming in to say I'm sort of in the same boat. My ER was 10%/PR - but Oncotype came back with ER negative (6.0 and the threshold is 6.5)/PR neg. My Onco score was 60.
I started chemo last Thurs. I think I will still be getting hormone treatment too but I'm waiting to hear for the pathology & tumor board review. But the guidelines I read here (I think BarredOwl posted them in another thread) say anything over 1% should get hormone treatment. I just think we can't count on it to be very protective so we need the chemo as well.0 -
You’re right about the guidelines Moth. My second MO shared that some years ago the recommendation was anything under 10% received chemotherapy but at some point that changed. I think all of this is confusing and they powers that be need to come to a clear decision
My first MO did not offer the Onco test. I requested it because I knew of other women in a similar position that received hormone therapy so I wanted to be sure chemo was the best choice. I needed more than just her recommendations to sell me on chemo. Just imagine if a woman does not know about getting an Onco score. She would never know if chemo would benefit her.
0 -
Hi ladies! I was 4% estrogen positive, progesterone neg, and her2 neg with a ki67 of 93%. I never had an oncotype done, but my dr ordered mammaprint, and it said that I had a basal like tumor and that I had a high chance for recurrence if I didn't do chemo. My dr said that even though I was 4% er pos, that my tumor behaved like triple neg so that is how we are going to treat it. I have finished chemo and had my lumpectomy, and will be starting rads soon. Because of that 4% though my dr is thinking about possibly having me take tamoxifen for 5 years. I wish there was consistent guidelines about tamoxifen.
1 -
I’m 5% ER positive 10% PR positive and her2 negative. My doctor is treating mine as if it were triple negative. I had a mammoprint done. I’m also BRCA negative. He said he may test the positivity again when we do surgery because it could be even less positive than it is currently. He said if that’s the case he doesn’t see hormone therapy benefitting me really to have to deal with the sideeffects from it
0 -
old thread but bumping both for participants & anyone who comes across this through seach functions
Almost 90% of "Low HR-positive" BCs (ER and/or PR 1–9%) are basal-like at the molecular level, and have a similar clinical behaviour to TNBC
https://www.sciencedirect.com/science/article/abs/...
0 -
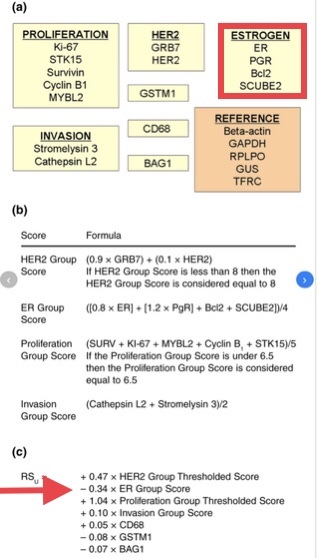
And I'll add that ER and PR are significant factors in the Oncotype calculation. The presence of ER and PR reduces the Oncotype total, so those with high ER and PR are more likely to have lower scores, while those with low ER and PR are almost guaranteed a high Oncotype score.
 0
0 -
Thanks for this, Beesie and Moth. I'm interested in finding out more about why my MO classified me as "TN" when my PR is 12%. Since I have IBC, I'm being treated with chemo, surgery, and radiation, but I'm wondering if there are any hormone suppressant protocols that might benefit me later. I see very few BC patients with ER-/PR+/HER2-.
0 -
Faithwalker I am weakly ER+, about 5 to 20 cells I think, so am being classified as triple negative with recommended chemo as the first line of tx.
0 -
I had less than 10% positive ER, and my MO theorized that my tumors were initially (de novo) triple negative. Somewhere along the way, some cells...very few, developed ER receptors. My Oncotype was 57. He classified me at Triple Negative but I am on five years of Exemestane now for the weak ER part of the beast.
0 -
I'm Er 100% pr 15% on path report but had an oncotype score of 51.i also had 3 positive nodes which altogether gave me 40% recurance risk on AI alone. I did chemo and am now on anasstrozole. But I'm wondering if it is doing any good at all
0 -
what is ki67?
Also I'm 2% er+ and treated as triple negative. How can I find out my ki67? And do you all know your subtype of tbnc? I wonder about mine. Or how we know if ours is in the 90% basal like category?
Erin
0

