Are you currently (or have you been) in a Clinical Trial?
Comments
-
Bev...yea it is only for Non Metastatic... So Moth that wont work for me. I really can't concentrate today my husband got a call that one of his Marines- wife has tested positive for Covid...so I am little out of sorts...right now.
0 -
luce..you should check again bc I did and the Pact is recruiting.
0 -
Nicole,
But are they only recruiting for those West Coast sites? Or are they going to set something up on the East Coast? I sent them an inquiry about this side of the country and they did not respond.
Thanks.
0 -
Nicole, When and where did you try? I talked to two sites today (SF and City of Hope) and they both told me the breast-cancer arm is closed. I talked to the trial nurses and the PI at both locations. I was told the breast cancer arm is closed everywhere.
0 -
Nope.. Irvine
0 -
National Cancer Institute article on approval of Keytruda for Tumor Mutational Burden - High:
https://www.cancer.gov/news-events/cancer-currents...
Interesting article also reinforcing the growing importance of genomic testing.
0 -
Nicole- Thanks for that link to Berzosertib!! Apparently all the drugs ending in "ib" are kinase inhibitors (eg, palbociclib, abemaciclib), as Berzosertib is an ATR kinase inhibitor. Seems to be remarkably strong and they are saying SEs seem minor.
ATR kinase is used by many cancer cells to repair their DNA, but normal cells don't depend on it as much- so this drug is going to push the killing of cells, as opposed to putting them to sleep. And the first phase one trial in ovarian cancer it doubled PFS over chemo alone- even worked on a patient resistant to PARP inhibitors
0 -
So, there are a lot of other implications for having a good ATR inhibitor available in the clinic. The phase one trial showed clinical efficiency higher in combination with chemo, and the breast cancer radiation trial mentioned above will test synergy of the drug with radiation-
Cancer cells treated with chemo or radiation that induce DNA damage can survive by upregulating PD1/PDL1, and ATR inhibitors prevent this. So this drug behaves similarly to keytruda in a way, and should synergize with some other kinds of immunotherapy. Its very encouraging to read about people taking it for multiple years already! hope they develop a pill form..
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC60791...
0 -
Reference..the link I posted...to bad its not available now...
 0
0 -
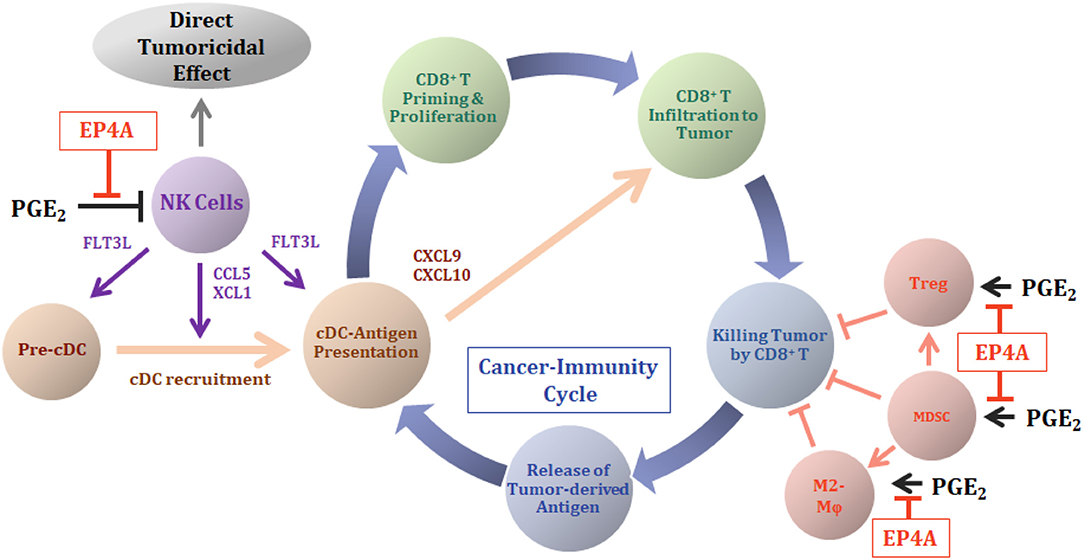
Luce, definitely anti-inflammatory drugs boost immune system killing cancer cells and response to immunotherapy- this is the basis of EP4 (next gen COX2 inhibitor) plus immunotherapy trials, its the action of these drugs on the tumor microenvironment rather than the cancer that activates the NK cells and gives this effect- so I am taking celebrex, and keeping an eye on that EP4 I-O trial
 0
0 -
Back for a moment to the California CAR-T PACT Pharma trial- they say future trials will increase the number of cancer-specific T cells they make to as many as four different ones (current trial is identifying and using just one).
However, we now know of the existence a universal cancer-specific antigen (present on all types of cancer cells and not on normal cells) which was identified last Dec in Nature, so will these trials also include that one? Hope it can be made widely available
A description of the overall technique from the company website
I thought most clinical trials shuttered down for new patient recruitment and are just treating already enrolled patients during covid, but is this going to put all our progress behind by a year now? or can they somehow catch up?0 -
Thanks to everyone for your recommendations and kind thoughts!
Cureious, Really appreciate your detailed explanation of the CDK 2/4/6 drug!
Hugs, Susan
0 -
HI!
my MO at MDACC said she checked with her colleagues in the trial department and thinks I could qualify for the CDK 2/4/6 trial NCT03519178 if I don’t take any more chemos (it allows 1 or 2) so it’s nice I could have something in my bucket IF I choose to go that route when my current line failsI also asked her about my MRE11a somatic mutation getting me into NCT04266912 which is only offered at MDACC. She did not check on that one.
We did talk about my having IGG deficiency caused by the cytoxin I took 7 years ago. I get infusions every 5 weeks of IVIG. Because the immunotherapy drugs are all based on IGG I asked if that would disqualify me from those drugs. She did not know that either. She said it is up to the individual trial. Grr.
Is anyone here on either of these trials?
I was offered to submit to UCSF for a Neuroendocrine trial NCT 03136055 that is basically Keytruda plus another drug. But that one is really far from home and requires a lot of days there to get infusions.
Navigating trials is tricky
Dee
0 -
Dee,
I agree that navigating these trials is very tricky. Since I've been on so many treatments, I am excluded from so many trials.
My MO suggested the CDK 2/4/6 trial but I have been on more than 2 previous chemos.
I previously failed on Pembro so can't do that trial.
Trying to get F1 done again (last one was 3 years ago) but in my last one only had PI3K, ERBB3 and TP53 somatic mutations. Already took Piqray and the other mutations don't have targeted treatments.
Last Thursday, she suggested the FORTRESS trial (Balixafortide + Eribulin). Anyone on this trial or know anything about it? The eligibility criterion is not very strict.
Hugs, Susan
0 -
Susan what is Balixafortide?
0 -
It's an immunotherapy. In reading more about it, it's a CXCR4 antagonist. As far as I know, I have no evidence of CXCR4 expression. I think that mutation is more common in people with bone mets. I had only one tiny bone met.
0 -
Susan,
Sorry you didn't qualify for the CDK2,4,6 trial, but if that drug is any good hopefully it will get expedited FDA approval, like Ibrance did
Balixafortide is the very promising CXCR4 inhibitor- it did so well in earlier phase 1 among heavily pretreated patients and I think increased overall survival also. CXCR4 is highly expressed in many tumors but also in immune cells that hide tumors from immune surveillance; so this is both a drug and kind of immunotherapy- the cancer cells will actually be getting killed during your treatment, not just kept asleep, and maybe thats why it improved overall survival?
For ERBB3/HER3, it has only weak kinase activity so the antibodies don't do much, so it must act in a different way. However, HDAC inhibitors have been found to reduce ERBB3 expression, so this is one way that you could treat it (if the cancer is dependent on ERBB3). The MORPHEUS trial is testing the HDAC inhibitor Entinostat together with immunotherapy, but I think it maybe for only 1st or 2nd line treatments? There are other HDAC inhibitor trials but Hope will know better about that...
https://clinicaltrials.gov/ct2/show/NCT03280563#co...
background info: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC64256...
0 -
PS Also, did you consider the PACT CAR- T trial? Very hi-tech immunotherapy and available at UCSF, seems not to have many exclusions?
0 -
Susan
I hope you can find a trial that works. I have the FORTRESS trial on my saved list. Are you just looking ahead like me or is your current treatment failing?
FYI- stupid Cancer treatments🤬
I take IVIG due to hypogammaglobulinemia from cytoxin from 7 years ago- knocked out my immunities. I asked a NIH doctor/scientist if this would preclude me from trying any immune checkpoint inhibitors (Anti PD1/PDL1). here is what she said.
“That is a great question. I'm not sure we know for sure if it would affect your ability to mount an immune response to the agent. However, a quick review of the literature proposes that IVIG may neutralize the anti-PD1 or PD-L1 antibody. Since we use IVIG to treat some of the neurologic toxicities, I suspect that this type of treatment may not be as effective for you.
I do think that most trials with antibodies that bind IgG4 like anti-PD1/L1 would potentially exclude you given this history and continued use of the agent.“
Thenshe said this about a trial that she had in mind for my Neuroendocrine Breast cancer “this trial does include an anti-PDL1 agent, I'm not sure that you would be eligible with continued use of IVIG.“
Now I need to go through my saved trials and cull them down. 😢Dee
0 -
This isn't strictly about clinical trials, but it intersects with clinical trials and treatment determinations. I am cross posting here and on liver mets thread.
I just watched an hour long webinar put together by the Cancer Research Institute, which promotes immunotherapy treatments. The webinar featured a scientist from CRI. plus two medical researchers from the Broad Institute in Boston (one of whom is a medical oncologist as well.) The hour long presentation talked about genetic testing as well as genomic testing, what the difference is, what the implications of each can be, and also things like liquid biopsies and their reliability and how all of this testing can affect what treatment decisions we should expect, and how we can push out MOs to use these tools in creating more personalized cancer medication combinations for us. It was truly fascinating, and an excellent use of one hour of your time, if you are interested.
0 -
Thanks for posting that bev...I will take a look.
0 -
hi NicoleRod
What kind of treatment you have being on right now ?? Im in the same situation like you
Is xeloda working for you ??
0 -
Andish, Failed Ibrance/Letrozole/Faslodex first....then I failed Xeloda, then failed Doxil..now today Eruibilin.
0 -
Bev. I watched the video... So my TMB is Intermediate and I am Microsatellite MS - Stable...which in the video sounds "like" I would be a GOOD candidate for immunotherapy.
It was really good.
0 -
That would be excellent, Nicole! And, consistent with not having strong response to Ibrance
one marker for responding to Halaven/eribulin from the EMBRACE trial was having high baseline absolute lymphocyie count ALC (≥1500/µL) levels- these patients experienced a greater OS benefit following eribulin treatment
PS "Microsattelite Instability- High" is relatively rare in most cancers, but when its found then people are eligible for immunotherapy as early as secondline, regardless of the specific cancer type
0 -
Good Afternoon Ladies, I just wanted to post an update on the trial I was on. Keytruda with chemo injections. Scans show progression again so onto the next one. They are talking about a trial with a ttk inhibitor. I'll have to do some research but if I decide to join I will update as trial goes on.
As always I hope everyone strength and good results. Although I dont post, I feel as though I know so many of you.
Kathy
0 -
Hi Kathy, sorry to hear the Keytruda & chemo didn't work for you & you have progression. I'll be keeping an eye on what you try next as I'm triple neg too. I'm curious - have you had fresh biopsies to confirm markers haven't changed? hugs
0 -
Hi Moth, thanks for the well wishes. I was happy to read it looks like your combo is working for you. I do not qualify for that combo, sadly. I'm sure with most recent trial biopsies I would have been checked. .I have not had any outside genetics except original to see if I had any mutations. None. I have been in 5 trials now with most successful being same one as Katie Smith. An ep4 inhibitor and immunotherapy. I will post again if I join the trial
Good luck with next scans
Kathy
.
0 -
HI Wereon.... Which chemo were you on with Keytruda? I see you are HER2- so how were you able to get into the trial it was for HER2- ?? Usually they are just for TNBC?
0 -
Hi Nicole, I am tnbc. I didnt have chemo with Ketruda. I had chemo injections into tumour 5 times with Keytruda. Sorry for any confusion
Kathy
0


