Starting Nerlynx in May, 2019
Comments
-
SP,
After years of abusing what my mother calls our "cheap Irish skin" through excessive exposure to the sun, in recent years I've become a crazy person with sunscreen, wearing it on every bit of exposed skin even when I never plan to leave the house that day--and three coats of three types on my face, trying to compensate! I cannot undo the foolishness of youth but I can be responsible now. Did you know that UVA rays come through any window in your home or car? UVB rays burn but UVA ages our skin. While I have not moved to SPF gloves while driving, I definitely wear a rash guard when I swim. Your information got my attention because prior to the quarantine, my fingers would crack constantly at the tips and my nails would split right down the center and even when I kept them short I could not keep them from doing it. Honestly, it seemed they would never improve because they almost seemed damaged. I knew it was the Nerlynx because I'd read it was common. Well, when the quarantine started I continued with my SPF but wasn't driving anywhere and things slowly improved. I was generally only outside in the evenings to walk. I never considered that my reduced sun exposure (thanks to Covid) was the thing that probably helped my hands heal. When it was at its worst, the only thing I found to help the skin cracking was liquid bandage. I still have some trouble, but nothing as before.
Some close friends of ours had a son with a Glioblastoma Multiforme IV at age 8 and after all other treatments failed, they tried Lapatinib (which is also sometimes used with breast cancer). He had such awful diarrhea he finally told his parents he did not want to take it any more. In truth, it wasn't doing anything for him at that point. The EGFR tyrosine kinase inhibitors can be very effective---but come with a myriad of crazy side effects. Wishing yours will become less of an issue in every way, dear Shetland.
0 -
Bumping for neeli, who was looking for a Nerlynx thread, and hoping she will find us here. So, neeli, you said you were starting with six pills per day, and wondering about side effects. Know that dose reduction, dose escalation (gradually going up from three pills), and a variety of anti-diarrheal meds are options. Watch the diarrhea and any vomiting carefully at the beginning, and stay in communication with your doctor and nurse. My newly assigned trial nurse did not explain very well what warranted a call, and did not check on me enough. So instead of pausing when I should have, I ended up needing to go to the hospital for fluids and electrolytes. This does not have to happen. Long story short, I am doing well on four pills per day, and since in my case it is for stage iv, we can see from my scans that the drug has been very effective.
0 -
Beesy, I wanted to respond to something you said here in September: “It's amazing how much things have changed since I first started reading about Nerlynx dosing until now--docs have finally realized that most women need to titrate up and they've also come to realize that six is not a magic number (it's probably just the most they can give you without killing you).“ I think that is literally the case. I have not researched the details of the early Nerlynx trials, but many trials use an old-fashioned, crude method of giving a very few patients the highest tolerated dose, and that sets the standard. This method is based on an old assumption, that began with chemo trials, that more is better. But that is not always true, for many reasons. See The Patient-Centered Dosing Initiative https://www.therightdose.org/
0 -
Shetland, I've actually been curious how much Nerlynx you were taking now, wondering if you would be able to stay on a lower dose on the trial. I'm thrilled to hear that you can and that it has been effective for you! I know I've said it many times, but reading of many women with MBC who had seen amazing results with as few as three pills daily made me persevere. I think of all the women who've quit because they just couldn't handle six a day when they might have done fine on a lower dosage. I'd seen the website you reference when Bestbird linked it a while back--hopefully this idea will gain traction!
Neeli, I would second ShetlandPony's comments about dose escalation! I know women who took six pills for a year (more or less without problems) but most of us can't say that.
0 -
Beesy,
Nerlynx is one of several meds that my MO is currently considering for me. Per F1, I have two ERRB mutations in my cancer.
My understanding is that neratinib is commercially available at this time, but only for trip neg BC. Otherwise, it's within a trial. I didn't read back, but I'm wondering how you were able to get on this drug without being in a trial and without being trip neg? I am hormone positive and HER2-, but with these HER2-related mutations.
Also, have you been able to get any assistance with payment for the drug, if I may ask? My understanding is that it's incredibly expensive commercially.
Thanks for any info you can provide. Trying to put puzzle pieces together.
0 -
BevJen,
Nerlynx was originally cleared for HER2+ early stagers (even before those with MBC) and is commercially available to us, whether hormone positive or negative. It's been a few years since I read about it thoroughly, but I have a memory that they did the trial with the idea that they could reduce the number of women ending up with MBC because HER2+ cancers like to go to the brain, and in my case, this is the only drug that I will have taken that crosses the blood brain barrier.
Nerlynx is pricey--the last number I heard was something like $14K/mo! My insurance has paid for it completely, but I've heard of other women who don't have the insurance I do getting assistance through the pharmaceutical company, and end up paying only $10/mo. There is a very active Neratinib Facebook Group (I'm not on FB but my daughter joined for me--there's a LOT of drama over there whining about side effects but there is also a significantly larger percentage of ladies with MBC). I never completely understood why the MBC forum here was separated out, but after reading the FB Group for a very short time I NOW UNDERSTAND COMPLETELY. One word: insensitivity. I digress.
You may have seen this by now, but ShetlandPony is taking Nerlynx (with success) for similar HER2-related mutations.
0 -
Beesy,
Thank you for your response. I really appreciate it. I am on Medicare Part D, and so I will get hit with a pretty big co-pay if/when we switch. Those reduced co-pay cards cannot be used with Medicare prescription plans, so I would have to try and get the company to reduce the cost for me. And yes, I do know about SP's trial. The closest one to me is a couple of hours away. My MO had told me that they were going to start up the trial at my cancer center, but that was before Covid hit. It hasn't started.
So we'll see how things go.
0 -
Yes, Beesy, I made two attempts at six pills per day. For the second attempt, I took a break and then employed four drugs for diarrhea and vomiting. Nope, couldn’t do it. I took another week off and informed my team that the only way I would re-start would be to titrate up from three pills. When a nurse said she did not know if the trial sponsor would allow it, I said it did not matter what they said, that was how I was doing it. With budesonide now on board, I took three pills per day for two weeks, still using the other side effect drugs to start, then went to four pills. And there I stayed. I weaned off the scopalomine, then the zofran, and eventually the budesonide; still use loperamide and occasionally lomotil. Hearing from you and another person about people having success on lower doses was really helpful to me. I found out later that the sponsor had tried to kick me off for getting so sick at the beginning, but my onc fought for me, and now I’m making their drug look good. You just can't give a pony such a high dose.
Hi, Bev!
0 -
Good for you, SP, for sticking to your guns and insisting that this is the way it was going to be. There was a gal on here named HomemadeSalsa (who is long finished with Nerlynx now), who's MO suggested from the start that she take four pills. She was the first one to get me wondering if this "one size fits all" approach wasn't a fool's errand.
BevJen, give me some time to find the information on Puma's assistance program. I looked a bit earlier today but couldn't put my fingers on it.
0 -
Hi! I heard my name called... ya, my MO agreed that 128#me was not the same as other bigger gals. I went 2 to 3 to 4 over several weeks and some Colestipol. Never needed more than a couple of imodium, and finished almost a year before I quit in April to get my knee replaced. Ate whatever I wanted after the first few weeks. I was terrified to start but it was easy. Really.
0 -
HomemadeSalsa---Great to see you around here! 😊 Yes, you were the first one (via your MO) to mention a lower dose. Since that time, I've read of many MBC women on as few as three who are NEAD. Glad you are well!
0 -
BevJen,
I finally had some time to look for the site that describes Puma Biotechnology's site describing their reimbursement program. I have read about at least thirty women receiving their treatment for $10/month. This site explains the co-pay support but also supplies a phone number where you can talk to someone.
https://nerlynx.com/access-and-support/access-programs
Sorry this took so long.
0 -
hello 👋 I’m new to this thread - I have been on Nerlynx for 2 weeks - taking only 3 tabs - to increase to 4 on my 3rd Week - I have what feels like constipation my 1st week so I lowered my dose to 1 loperamide/Imodium - last night and this morning wasn’t fun - the diarrhea is not bad it’s the abdominal cramping - I took 2 more Imodium and chased it down with lomotil as I have To work - Anyone ever just took 2 tabs of the nerlynx And was ok? Still had the benefit? - I muscled my onc into starting me on this - like throw the kitchen sink at me - and I think the recent data coming out convinced him - anyone on Bentyl/dicyclomine? To help with cramps
0 -
FNPMom,
I am not familiar with the drug you mention for cramps nor have I read of anyone using it, so I cannot speak to that. Could it be that you're taking too much Imodium (I know it's scary to back off)? The one thing I would say is that while I'm hardly the poster girl of dealing with Nerlynx well, most people acclimate over time, so I'd hang on if you can. But if I were you, I'd ramp up slowly and after each titration, give your body time to adjust. Does it feel like constipation or is it constipation? When I was at your point in the process, a friend with IBS (suffers from diarrhea then resulting constipation) told me that Miralax was her best friend, so even though it sounds crazy, I tried it and it did help. Prior to this, I was on the "Nerlynx Swing" as I called it--Big D and then Big C--until the Big D came back 😬. When I mentioned taking Miralax to my MO, he suggested I try Psyllium husks instead because it's a little more bulk-forming but will keep things moving. I take four Psyllium caps daily at night and have most of this year. For what it's worth, I have gotten up as high as five Nerlynx daily but eventually end up back at three daily and the last time I have just stayed there. I still take at least one Imodium daily. Like I said, I'm not exactly a poster child of great success in terms of side effects, but I'm six weeks away from taking it for a year and am grateful to have had the opportunity. I know of ladies with MBC who are on as few as three pills daily and are NEAD on that number. Before I started Nerlynx, it was six pills or nothing and only within the last year or year and a half have MO's started to consider that lower quantities may be effective.
0 -
FNP - I did pretty well on Nerlynx so I'm not sure I can make a ton of suggestions, but if I were you, I'd:
1) be careful with diet for the next few weeks as the body acclimates to the drug
2) cut down on the lomotil - only take it if you have diarrhea
3) if those ideas don't work, then cut back to two pills for a couple weeks then come back up to three
If you're still having problems in 3-4 months, you have to decide whether to live with them or quit the drug. Some people just have a hard time with it, some don't, some have a rough start and get used to it. I personally had a pretty easy start but it seemed to get harder (more bloating and cramps) as the year wore on. I did finish though and consider myself to have had minimal side effects while continuing to eat whatever I wanted.
I am finding now that after 4-5 months off the Nerlynx, I am not able to eat the way I used to without gaining weight. While I didn't have much diarrhea (maybe a day or two after I stopped and restarted at my PS's direction), I did have very regular, fairly gassy and explosive BMs. I have always tended toward constipation though. So it's back to the uber healthy, high fiber eating that I was doing before cancer. No more waffle house for me
 0
0 -
FNPMom, I wanted to say hello to you. I am currently on neratinib, managing pretty well on four pills per day. Six pills per day was a spectacular fail. If you get constipated, be careful about suddenly abandoning all the anti diarrhea meds as things may swing the other way. I think there is a lot of hope that you can do three or four pills. It takes some time for your body to adjust and for you and your doc to work out the right meds to help. For a while I needed Imodium, zofran, scopolamine, and budesonide. Currently I am only using immodium. Maybe a lomotil once a month. Also remember your BRAT diet and its opposite.
0 -
thank you for your responses - really appreciate it - I think I adjusted way too early - I was taking 2 Imodiums then when I had constipation I decided to take only 1 with the next dose and then I had diarrhea - I had constipation with kadcyla which is why I over reacted - think I have it back to normal or as normal as I can have it - I’m supposed to go up to 4 now but I dread it - I will psyche myself and just do it - I’m considering asking my onc for cholestramine - at least it will have the added benefit of controlling my lipids - I hope everyone well
0 -
My onc wanted to see me doing well for two weeks on three pills before moving to four pills. How long have you been on three, FNP?
There are three drugs the pharmaceutical company suggests. I was given immodium and budesonide, and also lomotil. It looks like the cholestramine you mention would be related to the colestipol below? I don’t know why, but my onc does not even glance at that one. Maybe there is a reason she does not like it for me. From the Nerlynx web site:
ANTIDIARRHEAL PROPHYLAXIS
Diarrhea management should be started with the first dose of NERLYNX1 Medications that help manage diarrhea have different mechanisms of action; if one doesn't work, another might Dietary changes or NERLYNX dose modifications may also help manage side effects1If the patient experiences break- through diarrhea, consider modifying, adding, or replacing one of the antidiarrheals1
MEDICATION
MECHANISM
Budesonide3
Anti-inflammatory
• Glucocorticosteroid with substantial first-pass elimination
The formulation contains granules that are coated to protect from dissolution in gastric juice, but dissolve at pH >5.5,ie, normally when the granules reach the small intestine
Colestipol4
Bile acid sequestrant
• Colestipol hydrochloride binds bile acids in the intestine, forming a complex that is excreted in the feces
Constipation is the most common adverse reaction of colestipol treatment Take colestipol ≥1 hour after or ≥4 hours before NERLYNXA voucher program for a FREE 3-month supply of antidiarrheals is available for all patients
Loperamide5
Antidiarrheal
Opiate receptor agonist that binds to μ-opioid receptors in the large intestine Inhibits the release of acetylcholine and prostaglandins, reducing propulsive peristalsis and increasing intestinal transit time Reduces daily fecal volume, increases the viscosity and bulk density, and diminishes the loss of fluid and electrolytes0 -
FNP - I was also told two good weeks at x pills before going to x+1.
0 -
Hi ladies,
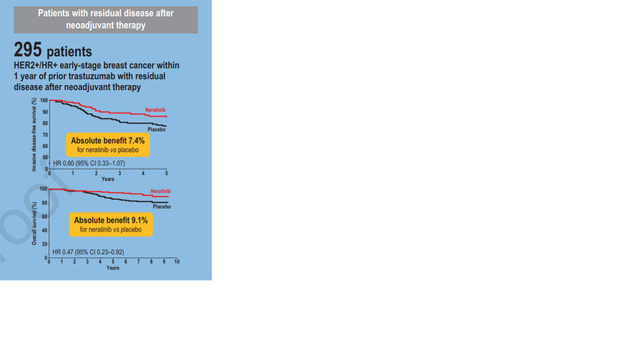
Checking in, 6 months after finishing Neratinib. I confirm it is easier to gain weight now. Just two weeks ago they published the results of the Extenet III trial; for triple positives with residual disease shows absolute benefit in overal survival at 8 years of 9.1%, that's pretty good. Even if the study was not powered for this type of subgroup analysis, there is a there there. Here is hoping for long years of extended health for all of us!
LaughingGull
 0
0 -
hello all - I’ve been on 3 tab x2 weeks - afraid to start 4 as I’ve doing so well x 2 days and only had to take 2 Imodium prior to the nerlynx - did anyone have to take Lupron shots? My onc moved me to anastrozole as I haven’t had a period when I was on a year of tamoxifen - but my estradiol is still at 48 - will it benefit me to have a total hyst instead?
0 -
Generally there is a choice between Lupron for ovarian suppression, and oophorectomy. A total hysterectomy would not be necessary for the aromatase inhibitor therapy. (Sometimes there are other reasons.) Your oncologist does know that absence of periods during tamoxifen treatment does NOT necessarily mean the woman is post-menopausal, right?
0 -
I've been getting Zoladex shots but I haven't had one since mid summer; we're checking to see if I'm in menopause. And yes not having a period doesn't mean you are post-menopausal. A total hysterectomy seems like overkill to me, but of course like all things it depends on your personal medical history.
0 -
The estrogen is produced in the ovaries, so to lower the estrogen the surgery would be oophorectomy i.e. removing the ovaries. That will put you in menopause, but would not prevent estrogen being produced in other parts of the body, which is why one still needs estrogen-blocking medication after an oophorectomy; to be discussed with an oncologic gyn, since removing the ovaries can create problems of its own.
Hysterectomy is a removal of the uterus, my understanding is that a "radical" hysterectomy would remove the ovaries too, but you can have a hysterectomy without removal of the ovaries, in which case your ovaries would still produce estrogen.
0 -
lol yes I think he does know that absence of menses doesn’t mean I’m no longer producing estrogen - it was a question of whether to keep me on tamoxifen or move me to an AI - I was concerned as my endometrial lining was thick to begin with - I wanted a hyst if he had kept me on it and even though AIs don’t feed the endometrial lining as much as tamoxifen - uterine cancer is still a risk with it - ah I’m just over thinking things - anyway I’m on 4 tabs and no diarrhea - so I guess that’s a win and the Lupron shot yesterday was ok - I’m actually tolerating the AI better than the tamoxifen or maybe that was the Kadcyla too 😊 I hope everyone is well
0 -
i hear you. Uterine cancer runs in the family so I'm hesitant about on it long term. I also think if I need oophorectomy or a hysterectomy (for one reason or another) I should just take it all out (radical hysterectomy). One less thing to worry about.
Glad you're doing well on 4 pills!
0 -
hi guys - so far so good - I'm taking 4 with 2 Imodium and when I get constipated I just take 1 Imodium with the nerlynx and 24 hours later I get one time watery results - then I go back to my regular regimen 😊 my onc said we'll try 5 pills after 4 weeks
I had a PET scan in the very beginning prior to all treatments and it was negative except for the cancer in my breasts - no imaging since - and he doesn't want to do one - except for the dexa scan as I'm being given Lupron and anastrozole - what about you guys any scans after treatments
0 -
FNP - I get no scans, and I even had some lung nodules at the get-go. After three inconclusive scans of those my MO is not recommending any more scans. My RO tried to schedule one and I cancelled it. Maybe after a couple years off the Herceptin and Nerlynx I'll scan again, but since there was no result that would tell me it definitely wasn't cancer, and since apparently catching mets before you have symptoms does not improve survival, I didn't see the point. Also, it was extra radiation and I have had more than enough radiation. And I've got other things to do.
LG - I'm carrying ten extra pounds and it will not budge. I pulled on a pair of winter pants this morning and I could barely get them buttoned!
0 -
Hi all, I thought I could report my short experience with Nerlynx so far... I've nearly finished my 2nd bottle.
My MO wanted me to start with 6 tablets a day which I refused and told her I read a lot about titrating up. I even printed the Puma study regarding control for her.
I started with 3 tablets a day and 1 Imodium. I had to stop the Imodium after 2 days, it made me constipated. After one week I went on to take 4 Nerlynx + 1 Imodium and finished the week like this. Then 5 Nerlynx + 1 Imodium the next week and I think I took one or two Imodiums during the week apart from the one with N. But I finished the third week uneventfully. The fourth week, I started with 6 Nerlynx + 2 Imodiums, but the Imodium was too much. After a few days I went to 1 Imodium and I dropped the Imodium altogether after about a week. So, all in all, my first month was quite OK. I started to feel tired about 3 weeks in, so on 5 tablets. Dozed off with the kids and woke up in the morning, which happened a lot during chemo.
My second month saw some D, even big D. I wasn't taking any Imodium. I think there must be some trigger food, but I was not able to pinpoint it so far. I had 2 episodes of D during the month. The first one started with rambling and then very watery BMs, like every hour, but I was distracted and somehow thought it would go away on it's own. Well, it didn't - after 2 days it dawned on me I had to take the damn Imodium, I don't know what I was thinking. The D stopped quickly after 2 Imodiums and 1 for good measure later. (Needless to say I didnvt have a BM for about 3 days afterwards). The next episode of D was very shortlived (about a week later), since I was paying more attention. I took 2 Imodiums right away, and that was that. Finished after a few hours. No other issues during my second month. The tiredness is subsiding.
So maybe this might help someone. Titrating up really helped me a ton.
0 -
JaBoo,
You sound like you've done very well on the whole! The trigger foods seem to vary from individual to individual but lettuce of any sort is definitely a trigger for me, for what it's worth. Good for you for sticking up for yourself regarding titrating up!
0