Biopsy results verses Oncotype results

My biopsy result was Stage 1A, node negative, ER+, PR- and HER2-. My Oncotype Dx report after surgery came back as single gene score with it now being triple negative. Which one is it?
Comments
-
There seem to be quite a number of women who've experienced the same thing... they are ER+ on their biopsy but ER- on the Oncotype. Or they are highly ER+ (90%-100%) on the biopsy an but very low ER+ on the Oncotype. PR- tends to drive up the Oncotype score and when that's compounded with a low ER, the scores are usually quite high. To my understanding, the pathology assessment trumps the Oncotype assessment (so if there is any ER, endocrine therapy will still be an option) but that doesn't change the fact that the low ER was used to determine the Oncotype score. The difference between the pathology and Oncotype assessments is definitely concerning.
What was your Oncotype score?
There are a few women who posted in the following thread who faced the same situation as you: https://community.breastcancer.org/forum/96/topics/869877?page=1
0 -
Sorry you find yourself here Abbidoodle, and with this kind of uncertainty.
Great advice and questions from Beesie. When is your follow up appointment with your treatment team?
0 -
Thanks for responding, Beesie. My Oncotype score is 41. ER score 5.5, PR score 4.1, HER2 score 7.7. Ki67 score high. I had an appointment scheduled for tomorrow 5/17 with the radiology oncologist to set up my radiation treatments, but was told they were canceling it and for me to see my oncologist. I have an appointment with him next week, so I'll have quite a bit more information by then. My surgery was over a month ago, and because the pathologist did not get my specimen sent to be Oncotyped, until 2 weeks after my surgery, I am just now getting my score. My surgeon had assured me before this that since my tumor was small (1 cm) he was sure I'd only need radiation and estrogen therapy. I've done very well with all of this, but was not expecting any chemo. I was diagnosed in February.
0 -
Abbidoodle,
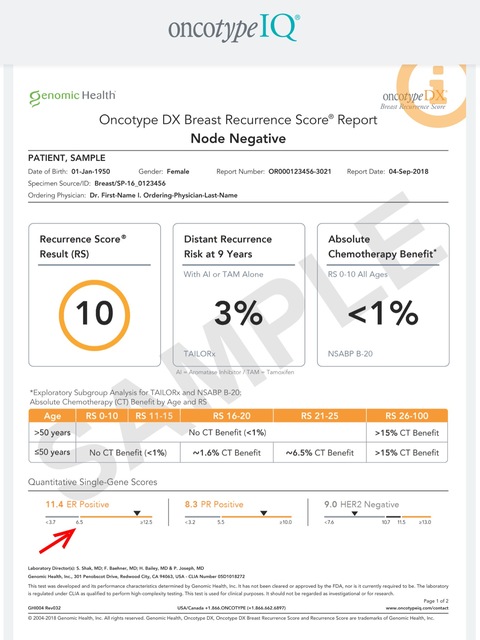
Although the Oncotype test considers you to be ER-, it is pretty close, as the sample report below shows. Do you know what % ER+ you were on your pathology?
In addition to the Oncotype score, the other factors that have been proven to be predictive are age, tumor size, and tumor grade. Even with a high Oncotype score, metastatic recurrence risk might be low if those conditions are favorable, i.e. the patient is older, the tumor is small, and the grade is low (1 or at most 2). Alternately, if those 3 factors are unfavorable (young age, large tumor, grade 3), one's risk might be higher than the 'average' risk indicated on the Oncotype report. In fact, while Genomic Health provide one set of generic results with the Oncotype score, there is a computer model that Genomic Health have provided to some Medical Oncologists that incorporates these factors with the Oncotype score to provide a more personalized recurrence risk estimate. I don't know if any of those factors are favorable for you (it sounds as though your tumor is smaller than average, so that's good) but this is something that you might want to ask the MO about. The computer model is called the Oncotype RSPC (Recurrence Score Pathology-Clinical).
0 -
Thank you for your input. I'll post an update after I talk with MO on Monday.
0 -
I too have a conflict. stage 1a grade 2 e-p p-n her- idc I noticed Onco said Her neg at the bottom of front page. I asked surgeon she said its pos. I asked a doctor that covered my radiologist while he out and he said it's pos. Then had results from a consult that ran their own pathology and the results were neg. I chose radiation until I decided to get chemo or not -ok with my onco doc. Rad doc returned and looked over the consult path report and said he believes its neg
My onco score was 35 so everyone wants chemo. This finding changes the need for aromatase if neg. I need to find out if this changes the chemo cocktail also. Have not decided on chemo as of yet. I will talk to onco doc Monday.
I'm scared to death of chemo and already have problems (low bone mass, neuropathy, fibro brain, prone to gum disease--which I have spent a small fortune to clear up, degenerative disc disease ). My surgeon was sure after my lumpectomy I didn't need radiation she told me and my boyfriend when I was ready to leave or. I appear to be healthy and was told by several doctors "your young and healthy should handle chemo well'" What ??? I took alot of time phys rehab and dietary changes to be a functional person. I would like to stay independent as I am single, no children, 2 brothers out of state and a few friends. 61 yrs old if that matters
Is this common with lab results and if anyone had this happen what was the result? I am so upset that besides being torn about chemo or not this er status is up in the air!! Anyone use a tumor board to decide?
0 -
Doubting-cw, your Medical Oncologist is the expert who should be explaining your pathology. And you should have a copy of the detailed pathology report so that you understand what he is telling you and can see it for yourself on the report. Do you have all your reports?
Is it your ER status that is uncertain or your HER2 status? The early part of your post seems to be talking about HER2 but at the end you mention ER.
If it's HER2, there are two tests that determine HER2 status. The IHC test is usually done first. If HER2 results on the IHC test are equivocal, which often happens, then the FISH test is done. This provides the final word on whether your tissue is HER2+ or HER2-. So it could be that your doctors are providing inconsistent results because both tests were done. Speak to the Medical Oncologist to get clarity.
If it's your ER that is uncertain, each of the pathology reports you've had done (including your biopsy report, if you have one) should provide enough detail (% ER positive) for your MO to be able to determine if an AI would be beneficial.
As for the 35 Oncotype score and the need for chemo, what was the size of your tumor? There is a model called the Oncotype RSPC (recurrence score pathology-clinical) that Genomic Health (the Oncotype people) make available to some Medical Oncologists. This model takes your score (35) and adjusts the recurrence risk based on your age (61), the grade of the tumor (grade 2), the size of the tumor (??), and whether and what type of endocrine therapy you will be taking (Tamoxifen or an AI). Your age and the grade will likely lower your recurrence risk estimate versus the standard number you receive with your Oncotype result, but the size of the tumor is also an important factor. Of course if you are ER- and won't be taking an AI, then chemo becomes the only tool in your arsenal.
0 -
My oncologist said that my path report was 7% ER+. He will be putting me on the drugs with the small chance that it might help. I started chemo last Thursday due to the oncotype of 41 and the grade 3. The plan is 4 treatments (every other week for 8 weeks), then 12 chemo treatments once a week then 4-6 weeks of radiation therapy, then hormone therapy. I'm participating in a nausea medicine clinical trial and also blood tests for them to freeze. Biggest thing I dread is hair loss, but grateful that my tumor was found early. If I can help anyone out with anything, please let me know.
0 -
Thanks for your post.
I am HER2 neg /estrogen on path report 5.9 pos/pr neg. Stage 1a grade 2 Tumor 1.2cm. Sorry I wasn't very clear about what concerns me . This diagnosis has me rattled and then the estrogen from the consult showing negative floored me. That's triple negative and chemo for sure. To have rad doc declare he believes neg is correct really made me think he was out of his specialty. He worked with the consulting MO at the U of M so I think they consult although he's now in a dif health system. They both know I don't want chemo as it only "may be effective". I was prepared to tell my MO no chemo just AI. Now this. Maybe their there in cahoots wanting the chemo.
I know I will have to ask my doctor what you suggested on Monday No the Oncotype RSPC was never mentioned and only met with my MO twice. 1st she ordered blood work and the Oncodx. Waited for results and talked on the phone. That's all.
You have given me a plan of action and now I feel much better. Thanks!!!
0 -
Hey Doubting-cw,
If you are not feeling confidence/trust in your docs, or even just feeling like they are not explaining things clearly - that is a good reason to get a second opinion. Almost all insurances will pay for it because cancer is expensive for them long term that they really want to get it right. If you have an NCI designated cancer center nearby (if you are in the USA), those are usually recommended.
I'm sorry you're having to deal with this. No one wants these kinds of nasty surprises. It's great that you are asking questions and empowering yourself.
0 -
Thanks for responding.
The second opinion Est neg was done at Univ of Mich Rogel Cancer Center which is NCI designated on the website I looked at. Running their own pathology was routine when I went for a second opinion in April. The doctor did not have the results at time of consult and it was never addressed again until I really looked at the Onco Dx report and saw they had me as neg for Est. I called U of M and asked them what their patho showed. That is when they ran it (took about a week) The pathologist called and told me the results. Neg for Est.
So much for my inquiring mind wanting to know. Will call MO in the am (todays Sunday) and find out. Makes me wonder if woman are getting the wrong treatment with this kind of thing happening. Imagine taking aromatase for years that wasn't needed.
Thanks so much for responding ! I do feel better knowing people like you are out there and very helpful.
0 -
doubting, I'm sorry u are dealing with all of this. I was pr neg on both path and oncotype. Strongly er pos on path but not very strongly pos on oncotype but still above the cut off. You are right, I would be alot more excited taking the little pill if I was more strongly positive. I'll have a year of AI under my belt as of this week. Keep us posted on what you find out from your MO tomorrow. Hang in there.
0 -
Hello again. It took a few days for my Mo to get back to me. She is sure my ER is positive and explained the difference depends on the sample. That's a relief---not triple negative. Beesie you made a really good point about the communication between patient and Mo. All I was told is Onco Dx result and sent for extensive blood work and need for new bone scan (osteopenia may have become worse). Can't get scan until next month because insurance pays every 2 years not a day sooner! This Mo was recommended by my surgeon (who is great at explaining everything). Total opposites!!!
Will make appointment to see Mo to get into Onco RSPC, discuss AI. I am staying with conventional treatment course.
Thanks ladies your responses really helped me calm down. I was a real mess when I first posted.
0 -
Doubting, Here are a couple of studies comparing the basic Oncotype recurrence score to the Oncotype RSPC. The first study found that more patients moved into the low risk category when age, tumor size and grade were factored in, whereas the second study found that more patients moved into the high risk category when these factors where considered. Although the studies had different results in this way, what is important is that both studies found that the Oncotype RSPC does change the risk assessment, and therefore the chemo decision, in a small but significant percent of cases.
https://ascopubs.org/doi/abs/10.1200/jco.2014.32.15_suppl.570
https://www.ncbi.nlm.nih.gov/pubmed/29128896
Given your age, the fact that your tumor was grade 2 and relatively small, and your 35 Oncotype score, I think getting the additional information from the Oncotype RSPC assessment is pretty important. Here's one case where this additional information made a difference in the chemo decision; see the July 18th post from TomMorrow
https://community.breastcancer.org/forum/109/topics/865972?page=1#post_5243967
0 -
I think being PR negative has a big role in the score of 35.
0 -
I'm not sure if my experience will help, but I'll add it just in case. I met with my medical oncologist for the first time yesterday and I had a similar situation. The tumor pathology after the surgery confirmed the initial biopsy pathology that it was 90% ER+, 90% PR+, and HER2-. Then the Oncotype comes back with a score of 24 and PR-. WHAT?
So I ask the MO, and she explained that the PR- represents a segment of what the pathologist determined was the most aggressive part of the tumor. She said few tumors are homogeneous. So essentially, as she said, a small part of the tumor was getting "smarter" and more aggressive. As mentioned above, that PR- aspect of the most aggressive part of the tumor drove up my Oncotype score. Since I am over 50, I am still spared chemo. But it was closer than I or my breast surgeon thought it would be given all the other factors. Thankfully, they are favorable (except maybe for age. I do not consider myself old!)

So yeah, it was confusing. I hope the above helps.
0 -
I had a er+ 95% and pr negative situation in both my tumors they were slow growing low grade but oncodx came back with a score of 34, I was 53. I didn't do chemo that was recommended I did do 4 years on AI drugs. I am 8 years out NED.
0 -
Momto I'm happy that you were spared chemo. This neg/pos difference really had me going ??? Thanks.
At the top of my onco dx it clearly states "Oncotype Dx analysis of ER expression indicates this specimen is ER negative The specimen must be ER positive by RT-PCR or IHC for the recurrence score result Clinical Experience to apply"
I have a list of questions for my MO that I am taking to her and would like answered-- and Beesie mentioned the Onco RSPC to be run so that is on the list as it may change the result. Hopefully lower the RC number.
For a small tumor that wasn't detected by my OB/GYN (had my annual the week before the mammo with breast exam) and my examination that's my habit when showering the abnormal mammo was the scariest part of this . My surgeon upon waking said no radiation in her opinion. Then to Onco surprise high score.
Meow the PR score sure did up my score I'm convinced especially with the statement at the top of report. Being 8 years out is wonderful-- hope I can write that in 8 years! I won't be doing chemo either. SAs are too much. I already have osteopenia, degenerative disc disease, lumber spine trouble and Fibro. It's imperative to keep my independence. The quality of life is most important to me.
I'm calling my MO office to try for sooner appointment I don't want the 3 weeks out wait.
Thank you so much.
0 -
For anyone who is interested, you might find the following thread helpful;
"Long term high oncotype test survivors"
(I just bumped up the thread to show it as active...or you can do a search for it)
My oncotyoe was 46. I found the thread helpful..
0


