Chemo or no Chemo? 😬

Hi Everyone,
I am 30 years old and was recently diagnosed with stage 1A breast cancer and had a double mastectomy about 3 weeks ago. I just got my results back for the oncotype and the dr recommends chemo. The score came back 19 out of 100, which means there's a 6% chance of it coming back, but that percentage doubles every 10 years So since I was 19 out of 100 she said the chemo would lower that percentage by 1. The type of cancer I had only responds to hormonal therapy which is why they did not recommend chemo in the first place and all of my genetic testing came back good.. so I am not sure what to do.. a lot of people are saying not to do chemo saying the benefits chemotherapy will not outweigh the side effects and some are telling me I should get it so I have no regrets. Has anyone else gone through this? Also, any advise or thoughts? 😬
Comments
-
CB, so sorry that you were diagnosed and have had to join us here.
Do you have your pathology report? More information about your diagnosis would be helpful to better understand your situation.
Your comment, "The score came back 19 out of 100, which means there's a 6% chance of it coming back, but that percentage doubles every 10 years" isn't completely accurate. For ER+ cancers, significant recurrence risk continues through to about 20 years, so the 9-year recurrence risk figure that you received from the Oncotype test certainly doesn't reflect your total lifetime recurrence risk, but your risk absolutely will not double every 10 years. It may double once, but at that point you will be approaching 20 years post-diagnosis and the risk from that point forward will be quite small (however there will always be some risk). So a 9-year risk of 6% might translate to something like a 14% or 15% lifetime risk, I would think. This is something you should get clarification on from your Medical Oncologist.
You also said that "The type of cancer I had only responds to hormonal therapy" which would not be true. ER+ cancers respond well to hormone therapy, but they do also respond to chemo. This is why for lower risk ER+ cancers, hormonal therapy alone is prescribed, but for higher risk ER+ cancers, both chemo and hormone therapy are recommended.
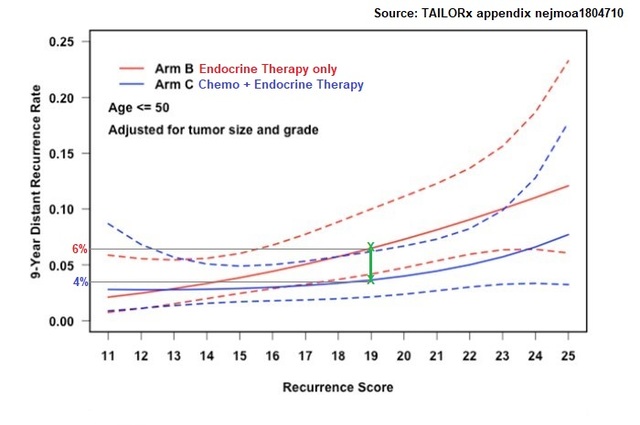
Lastly, about the Oncotype test. At your age, you fall into the "Under Age 50" category. From the TAILORx study, which is what the Oncotype recurrence risks are based on, it appears that for the average patient under age 50, a 19 score confers a 6% risk with hormone therapy alone and about a 4% risk with chemo + hormone therapy.
The issue for you is that at age 30, you are considerably younger than the average patient in the "under age 50" group, and age does matter. There is a separate computer model that your Medical Oncologist can run called the Oncotype RSPC Model (Recurrence Score Pathology Clinical). This model is available only to MOs; they can access it on their computers and it only takes 2 minutes to run it. The model comes from Genomic Health, the Oncotype company. What the model does is it takes your Oncotype 19 score and then recalculates your recurrence risk by factoring in your age, the size of your tumor and the grade of your tumor. The model then provides a new recurrence risk figure for your 19 score that is more specific to you. Your age, being so much younger than the average, would definitely cause your recurrence risk to go up from the 6%. I don't know your tumor size or the grade. If I recall correctly, the average tumor size is 1.75cm, so if your tumor is larger, that will also increase your risk, but if your tumor is smaller, that might lower the risk. The average grade is grade 2, so here again, if your cancer is grade 3, that will increase your risk whereas if your tumor is grade 1, it will lower your risk. Without knowing these other factors, it's impossible to guess what your RSPC recurrence risk would be with a 19 Oncotype score - whether it would remain at around 6% or whether it would increase - but I would strongly recommend that you ask your MO to run this model. If it turns out that your risk is considerably higher than the 6% average risk for anyone under age 50 with a 19 score, that might make your decision on chemo much clearer.
Hope that this helps. And please, let us know more about your diagnosis.
1 -
Oh gosh, you're very young.
I echo Beesie - much more info needed!Also, as Beesie says, there's no cancer that only responds to hormone therapy. You might want to read more about cancer treatment options on this breastcancer.org page https://www.breastcancer.org/treatment
Also who is the "some are telling me"? If you're getting discordant recommendations from MOs on your team or on 2nd opinion, that's one thing. If it's friends & family - that's a whole different thing. Same with our suggestions or 'advice' here.
IMO, bottom line is you have to trust your *oncology team*. I've had a situation where my team was unable to make a strong recommendation either way and they made a very weak recommendation but I could have overturned it if I felt strongly .... but usually, they have a recommendation and can explain the strength of the evidence they're making it on. It would take a lot for me to disregard it - maybe a second opinion from a top notch facility. Otherwise I listen, try to read up on it & understand their rationale (& realistically, the treatment protocols are designed by people with a whole lot more knowledge than I have about oncology, no matter how much I read & study the subject), consider if it's compatible with my goals (which are currently "as long as a life as possible") and if it's in accordance with the last point & appears reasonable, I do what they recommend. I really recommend people get a team they can trust - either due to personal rapport, willingness to discuss options or due to research affiliation and reputation etc.
I'm a no regrets / don't look back person so I did everything & more!
Oh, one other thing about hormone treatments - some people think these are easily tolerated and 'just a pill'. The thing is, they will put you into immediate menopause++++. There are plenty of women who have been unable to carry on with hormonal therapy because it interfered with their quality of life so much. They do cause adverse side effects. Many women are fine and manage them well but many do not. So that could be a problem down the road ... say you skip the chemo, and then can't tolerate the hormone suppression. Then you're back to relying only on your surgical benefit for long term survival.
You can try running your stats on the Predict website https://breast.predict.nhs.uk/tool
& see how many women with surgery only are alive at 5, 10, 15 years later, then add hormone treatment, then add chemo (you'd have to let us know which chemo they recommend and we can probably tell if it's 2nd or 3rd generation chemo)
best wishes
1 -
I chose to chemo with an oncotype score of 28 and my age was 64 at diagnosis. I wanted the certainty of having done everything I could to beat cancer. Chemo was doable, radiation was way easier than chemo, but the hormone therapy is throwing me for a loop with pain, insomnia and mental fog. Not sure I can take this for 5 years, but I'm trying.
0 -
My oncotype score is also 28. I had a mastectomy in October and chose to do chemo at 59. Right now I am taking Tamoxifen due to the osteoporosis, not so many side effects so far. I may switch to AIs later.
1 -
In hindsight, I am glad I did the chemo even with only a 2% or so benefit from it per my doctor, as I could not tolerate the AI route.
1 -
As other pointed out it very depend on your oncotype.
In certain cases of er+ and her-, preventive chemo is not suggested anymore, but in other cases it is...
Best wishes anyways!
1