Oncotype Scores - how do they determine the score?

Hi,
Looking for a bit of guidance. I had a BMX with SNB following DCIS 7cm diagnosis intermediate grade strongly ER positive.
The three nodes came back negative (yay!) for any invasive cancer following the SNB biopsy but they found 5mm of IDC (stage 2) post the surgery.
The IDC is ER/PR positive and HER negative so my PS has ruled out radiation. The next step is to do the Oncetype test to determine the recurrence score and if chemotherapy is recommended or if hormone therapy is enough. I have been told that the likelihood is that my score will be low based on my factors.
I was hoping to understand what determines the test. I know they measure 21 genes but hard to get any other information beyond this.
Is ER positive a good thing? What are the typical scores that are seen with IDC 3mm ER/PR pos and HR negative?
Thank you in advance for responses and wishing everyone the best and especially if you are waiting for results which is the worst part of this journey! :-)
Comments
-
Ava - Sorry I don't have answers for your questions, but it looks like you are HER2 negative. This is a HER2+ (positive) thread. You may want to delete & post in a different thread.
0 -
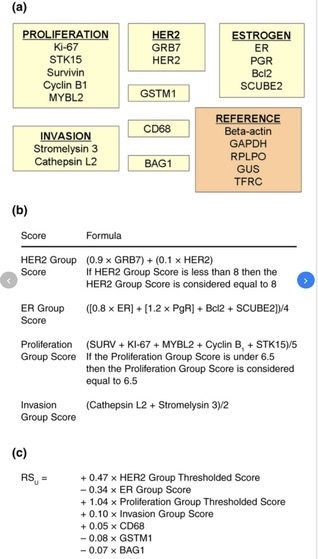
Here is the Oncotype formula. High ER and high PR are positive factors that will drive down a score.
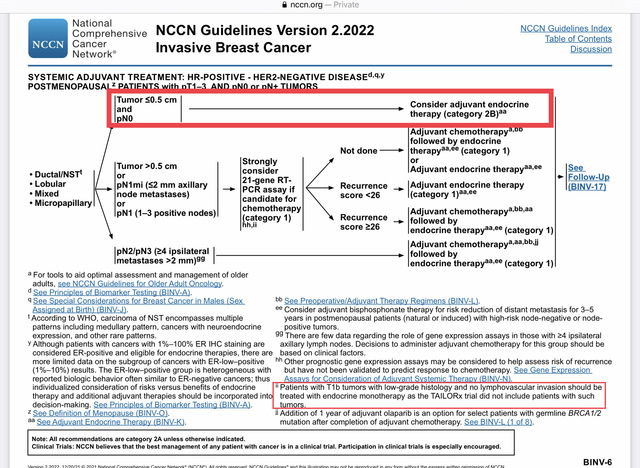
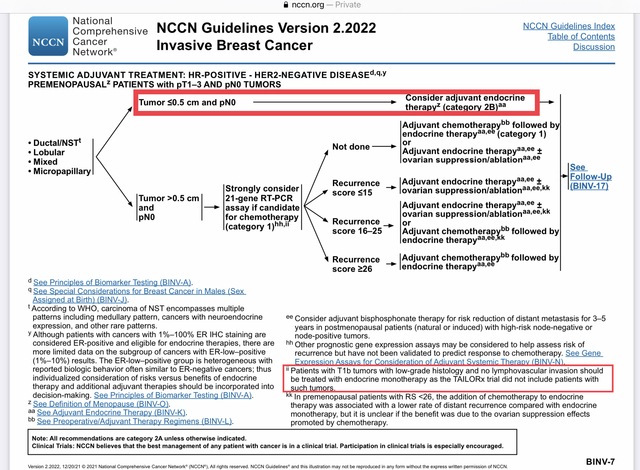
Is your IDC 5mm or 3mm? Normally an Oncotype is only recommended for tumors that are >5mm, and even then, you need to be cautious in applying the results because in the research that determined the risk percentages associated with each score (the TAILORx study), the average tumor size was 1.75cm - quite a bit larger than your tumor. Even for T1b tumors that are >5mm up to 1cm, the Oncotype test is not recommended if the tumor is grade 1. I believe yours is grade 2 (not stage 2), correct? In my case, my tumor was 8mm and grade 2, but it was just over the line to grade 2, a mix of grade 1 and 2 actually, with a mitosis rate of 1, and therefore my MO felt that I was so close to the T1b footnote (see the charts below) that the Oncotype results would not be representative for my tumor, and therefore we decided not to run the test.
Getting the information will be helpful and informative, but if your risk is intermediate or high (a high score is unlikely, I think), you need to be cautious in how you interpret the results given you have such a small tumor.
Here are the current NCCN Guidelines. I've included both Menopausal and Pre-Menopausal since I don't know your age.
 0
0 -
MinusTwo, just saw your post and noticed which forum this thread is in.
Ava, why don't you send a private message to the Moderators and ask them to move this thread to a more appropriate forum? They can do that easily for you.
1 -
hi Bessie!
I was hoping you would reply as I have been reading your posts over the last number of weeks and they are most helpful…. So thank you!
My IDC is 5mm grade 2 (stage 1) and I am pre-menopause age 49. ER/PR pos and HER negative. This was derived from 8cm of DCIS from initial diagnosis.
Does that mean I should get my pathology to see if I can get a bit more comfort around the reliability of the score? I would hate to get a high score and have to get treatment when it is statistically unreliable. What would you advise?
Also if I am strongly ER positive does that help drive down my score?
Thanks also Minus Two for spotting this too as I clearly posted in the wrong group and the moderators were in touch and said they would move it.
many thanks again0 -
Yes, strongly ER would help drive your score down. But there are many factors that go into the score, and you can see that the formula is complicated, so being strongly ER certainly doesn't ensure a low score. There could be something on the negative side that drives the score up.
"Does that mean I should get my pathology to see if I can get a bit more comfort around the reliability of the score?" I don't understand what you mean. The issue is the size of your invasive tumor. If it's 5mm, it's 5mm. As per the NCCN charts that I posted above, a 5mm tumor is just below the threshold for getting an Oncotype score, which is only recommended for tumors that are greater than 5mm. This is because there was no one - not a single patient - in the TAILORx study (on which the Oncotype results are based) who had a tumor that was as small as 5mm or less.
The analysis of the 21 genes within your tumor will be perfectly valid (assuming the sample sent to Genomic health is large enough to accurately analyze), so your Oncotype score will be correct. The question is whether the metastatic risk percentage associated with the score will be reliable; the reason that Oncotype testing is not recommended for those with 5mm and smaller tumors (or 1cm and smaller, if grade 1) is because an assessment has been made that the results might not be reliable.
It's logical, really. The average tumor size in the TAILORx study was 1.75cm. Suppose your Oncotype score is 16. That scores reflects the genetic make-up of the tumor. But suppose you have two patients with two identical tumors, both with Oncotype scores of 16. One individual has a 1.75cm tumor while the other has a 5mm tumor. Would you expect the metastatic risk of these two patients to be exactly the same? Logically no, because a larger tumor likely means that the cancer has spent more time developing in the breast before surgical removal, and that provides more opportunity for a few cells to break off and move into the body. However an Oncotype score of 16 will give both patients exactly the same metastatic risk assessment; even someone with a 3.5cm tumor who gets an Oncotype 16 score would have be given the same assessment.
If your MO is sending for an Oncotype score despite your tumor being only 5mm, my suggestion, regardless of the score, is that you insist that your MO run the Oncotype RSClin computer model once he has your score. This is a model made available to MOs by Genomic Health (the Oncotype company) that takes an Oncotype score and factors in the patient's age, tumor grade and tumor size, kicking out a new recurrence risk estimate. Very few MOs use this model, although they all have access to it and it takes two minutes to run. It will provide you with a more personalized recurrence risk based on whatever your Oncotype score turns out to be. RSClin: A new tool for 'TAILOR-ing' treatment in early breast cancer
Hope that helps.
p.s. It's Beesie, not Bessie.
0 -
Thank you so much Beesie your advice is verymuch appreciated!
0 -
Hi Beesie
I hope you are keeping well.
One further question that I was hoping you might share your expertise on. I got my pathology report back and the details are:
IDC NST -5mm, grade 2 (tubules 3, nuclear pleomorphism 3, mitotic activity 1)
Posterior margin: >10mm from IDC
Oestrogen receptor shows strong positivity in 80-100% of invasive tumour cells
Progesterone receptor shows strong positivity in 80-100% of invasive tumour cells
Her2 negative
I was hoping you might help me to understand if the above in relation to the grade is good or not so good (in the long wait for the Onctotype score).
Thank you again for your previous answers
0