Anyone starting brand drug, Enhertu?

I have had growth of tumors while on current treatment. My onc and I have decided to try new treatment, Enhertu (FDA approved 12/20/19)! Wondering if anyone else out there is trying or was in trial?
Julie
Comments
-
Julie,
I must google this as I haven't heard of it. Best of luck to you.
* Just googled it and it is for HER2 positive patients who have not done well on two other HER2 positive treatments at stage IV. It’s approval was fast tracked and was just approved in December . Will keep reading
0 -
Hi Julie-I hadn't heard of it yet either. From the website it looks like it for people who are HER+. Is that how your cancer has evolved? Keep us posted on how things go. I wish you the best of luck.
0 -
-
thanks, friends! Yes, did some research myself. Lots of possible side effects, but progression-free survival results were good!
I am unusual in that it appears I have Her2nu +,ER- Cancer In abdomen but ER+, Her2nu- in my lungs. (Based on biopsies)
My original cancer was triple neg. -has changed over the years. I am a “transformer”!
Also, recently found out I have the ATM mutation.
Thanks for the wishes!
Julie
0 -
hi julie, the Destiny trial of this drug is one I’ve been keeping an eye on since I’m HER2+ and have progressed on both HP and Kadcyla. But in addition to having some marvelous results, it has also had some serious side effects. Especially scary is interstitial lung disease (basically an irreversible scarring of the lung tissue) in 10% of trial participants... if my information is correct. Of course, we are always faced with cost-benefit risk analysis when choosing treatment so I’m interested to know the rationale of your MO in suggesting this drug. I’m not saying I think it’s a bad idea, I have no idea and with the potential benefits it may well be a great option. I’m just interested since I’m assuming that your treatment history in your bio is not up-to-date? Are your lung mets stable? Thanks and best wishes as you blaze ahead on this trail!
M.0 -
hi. there hasn't been activity on this thread for a little while, but I'm curious if anyone is taking (or has taken) enhertu?
0 -
hey, thanks for the reply. I believe my profile is now up to date. It is so long that the entire thing doesn’t show, however.
My lung mets (ER+, HER-)and abdomen mets (ER-, HER+)all grew some. My ONC felt I would do well on enhertu. He said it could have off target effects, so he thought it could work for both sets of mets. Enhertu specifically targets the HER2NU + cancer but is chemically bonded with a chemo drug also. (Kind of similar to Kadcyla), which I did well on for 3.5 yrs.
I started Enhertu Jan 29 and, so far, so good! Only had one episode of nausea and a little fatigue ( not bad, though!) haven’t experienced other side effects yet! Liking this one so far!
I am keeping very alert to the potential serious side effects, just in case!
Julie
0 -
hi Julie. Thanks for sharing your experience so far. Glad you are experiencing minimal side effects and I hope the drug works great for you!
0 -
jnh, glad to hear this drug has minimal side effects for you - hope that continues and that it is effective for you for a good, long time! Please keep us posted as I’m sure many of us are interested to know more about this new treatment option. All the best! -M
0 -
Jnh, thank you for posting your experience. I second MargaritaS's comment; we are many that are interested in this new treatment. Currently, it is only approved in the US, but hopefully it will reach the European market based on the currently available efficacy and safety data. The response rate in the trial is impressive, but as mentioned above there were potential serious side effects. Hopefully, post-marketing safety data and additional studies will support that this product is a favourable option.
I wish you every success with Enhertu, with minimal SEs, keep us posted.
Take care,
Meja
0 -
Julie, I hope Enhertu continues to work for a long time for you. I would really like to get on Enhertu for my HER2-low status. I look forward to further updates on your progress.
0 -
hi JNH - how are you doing? hope the side effects are still minimal for you on enhertu. have you had your second infusion yet? or is that next week? also, I'm curious, have you experienced any hair loss?
0 -
considering going on this-myself. Exttremely interested in side effects.
0 -
hi can this drug cause heart failure as I had this twice on hercepti
1 -
I will start this drug, Enhertu (Trastuzumab Deruxticans) this coming Tuesday, March 17.
I will try to post regupdates as to my side effects.
0 -
Miriam,
I wish you all the best with the new drug Enhertu, - and thank you for updating us on how you will be doing.
Take care,
Meja0 -
Today, I started IF (intermittent fasting).
Fasting has shown to help with autophagy and G.I. side effects afterward. That means I did not eat until lunchtime.
0 -
Day 1 - not too bad.
- Pre meds to give a 3-4 day fight off of nausea, Will keep you posted on that.
- 100 mg (?ml?) Enhertu Slowly administered to avoid HSR. None. Usually, will take about 1 hour.
I've been foolishly injuring my back with resting in the recliner, so have backache tonight & using heat pad & Ibuprofen. I never learn!
Decadron steroids (10 mg) have me ginned up still about 10 hours later. May have to take an Ambien. They had stopped my wheezing and coughing earlier today (not their goal) but the wheezing (very slight but I've got a 4x4 in my right lower lung) is now back at almost 10 hours later, LOL. Manageable, but a bit weird & not a good thing.
Will post tomorrow to answer some prior questions on this thread & update how I feel. Day 4 is usually my tough day, so Friday or Saturday may tell me the most.
be back soon
Miriiam (Corona Virus hot spot Montgomery County, PA) 0
0 -
Day 2: sleeping off the steroid sleep disruption today, so not much new to report.
Going back on Lysine (2000 mg/day) which previously always had 100% success preventing mouth sores (one of the SE's from anti nausea drug given in oral form, though mine was infused intravenously, but being proactive). Also, going back on Omeprazole since GI tract is affected by Enhertu.
No nausea yet. This web site has a really helpful article explaining Enhertu here: https://www.breastcancer.org/treatment/druglist/enhertu
Coughing has slightly subsided but this may merely be due to laying around so much. I have mets in several places, but the lung mets grew significantly between the break I took (my son got married in November so I asked to just stay on maintenance routine of Herceptin/Perjeta every 3 weeks). Oncs wanted me to start Halaven (Eribulen) in August but I asked to wait, since I already have some neuropathyand Halaven causes this as well. My neuropathy started while on Kadcyla (another more well-known smart bomb ADC), which pairs Herceptin with Emtansine. I had previously had a couple of taxane drugs (Taxol & later, Taxotere) but didn't suffer neuropathy from either.
Rainbow, you asked about heart failure from Herceptin. This drug is an ADC (Antibody drug conjugate) pairing Herceptin with, I guess, the strong chemo Deruxtican. As a smart bomb (chemoagent is hidden by the Herceptin) using Herceptin, you may well continue to have heart problems that you would have to discuss with your Oncologist. I have regular Echo Cardiograms since I've been on Herceptin since my metastatic DX (diagnosis) in late 2010. My ejection fraction always remains high, so Herceptin has been well tolerated by my heart. Still, I see an excellent cardiologist once/year. My Oncologist didn't seem to think that was necessary, but I chose my own path on that issue. I'm glad I did. I have good (expensive) insurance we buy as my husband is self employed.
I had hair thinning while on Doxil (April2018-May2019) and Enhertu will prob cause the same. We will see. I've got a good collection of “my girls" (wigs) on my shelf to use when my caps don't seem like enough. There's a few nice ones out there (I love Raquel Welch wigs & Amazon sells a cool hipster cap for which I have received a LOT of compliments...let me know if you want urls to either sites).
Will post tomorrow. So far, so good. I DO have an amazingly faithful prayer posse, a wonderful husband who will get me whatever, 3 great grown offspring who keep tabs on me (though, due to the Corona virus, are not coming to see me but texting, calling, etc.) & good genetics other than the Chek2 genetic issue (one of my tumor suppressor genes is defective). I will be 60 in August, have been fighting this disease for going on 10 years, and am planning a big party to celebrate if I make the 10 years in this condition.
Enhertu, I'm expecting big things out of you!
 1
1 -

Day 5 - I thought I posted a coupla days ago, can't see it here, oh well....it's been rather uneventfulTired today, so the fatigue is hitting...hard to do much today, though I was super busy vacuuming yesterday, but the house needs it right now. We have a very fluffy dog and 2 cats & they're shedding a lot right now.
Not much else to report...no nausea! Yay!
1 -
Thanks for sharing your experience with this new drug Miriam! I pray it works for a long long time xx
0 -
Daywalker! Thanks SO much! SO glad someone responded here because I wondered if there just aren't that many of us Enhertu girls. Based on your profile, you look like you're managing well with no evidence of disease. How wonderful!
And thanks mostly for your prayers. God has been very faithful to me for such a long time, and I am happy to be here or in the "next" body, in heaven.
Love,
Miriam (my daughter and me seeing Downton Abbey in September - yes, this is a wig I'm wearing, LOL)
 0
0 -
Day 12 - still tired, but figuring out how much black tea I can drink without caffeine SE’s (I’m highly sensitive to any/all stimulants). A certain amount of caffeine can help me keep moving, but too much causes major sleep disruptions. Combining a good walk with my daily routine is a big help. It makes chemo move through my system better.
No nausea!
Nothing else to report. “Making hay while the sun shines”, so am getting a few hours of “minor” help done on yard work. It’s raining all day here (SE Pa.) but getting mulch ready to spread on Monday. Due to COVID-19 precautions, not able to go places anyway, so it’s a great time to try & start up trimming & pruning.
We love our yard & seeing things grow in it. Coronavirus during the spring is tolerable, but we’re a bit nuts about wearing (& discarding) nitrile gloves.
(Miriam)1 -
This will be my next drug as my Oncologist and I have already discussed. I am currently on Xeloda and am doing okay . no lying ..xeloda is a brutal drug some days with the hand and foot syndrome and other SE's.
I hope everyone on the Enhertu is doing excellent. I was following the DS-8201 for a while then saw it was approved with name of Enhertu. I will be following this post.
Be well to all~
0 -
You can do it, DL3!
May I send you a helpful article? I'm totally stoked about this drug. No nausea (pre meds Emend & Aloxi/Dexamethasone saw to that).
I'm looking forward to success on this!
Miriam
0 -
thank you. I wont have next scans for about 3 weeks so hopefully this xeloda continues to work. I think I remember your name from the Kadcyla group?
Good luck to you sweet lady
0 -
Miriam, yes if you have a helpful article please send to me Thank you .!
0 -
(The following article is from www.onclive.com - Site requires you to register(free)/log in to read the entire 3-p. piece so I am including the entire thing here). https://www.onclive.com/publications/oncology-live/2020/vol-21-no-3/patients-with-her2-breast-cancer-gain-potent-option-in-thirdline-setting
Patients With HER2+ Breast Cancer Gain Potent Option in Third-Line Setting
Brittany Lovely
Published: Friday, Jan 31, 2020
A new drug is giving hope to patients with HER2-positive breast cancer who have failed multiple lines of therapy. Fam-trastuzumab deruxtecan- nxki (Enhertu) received a green light from the FDA in December 2019 after updated data demonstrating a confirmed objective response rate of 60.9% were presented at the 2019 San Antonio Breast Cancer Symposium (2019 SABCS). The antibody-drug conjugate is approved in the third-line setting for patients with metastatic HER2-positive breast cancer.
"We put up the waterfall plot at the meeting, and it really does take your breath away," Shanu Modi, MD, said in an interview with OncologyLive®. "You can see that almost every patient, even if they do not achieve a confirmed response, [gets] some benefit from this therapy. There are very few patients who don't have benefit outright."
Modi, lead investigator on the pivotal DESTINY-Breast01 (NCT03248492) trial and a medical oncologist at Memorial Sloan Kettering Cancer Center in New York, New York, spoke about trastuzumab deruxtecan's efficacy and potential impact on the treatment landscape.
Could you please provide an overview of the patient population?
The population for phase II of this study [DESTINY-Breast01] was built on the success of the phase I study that preceded it. The patients were those who had HER2-positive metastatic breast cancer who had previously received treatment for their disease; specifically, patients had received treatment with T-DM1 [ado-trastuzumab emtansine; Kadcyla], which is one of the most active therapies for HER2-positive breast cancer.
Ultimately, we ended up enrolling patients who actually had a median of 6 lines of prior therapy. They had a number of treatments, and all patients did in fact, receive prior trastuzumab [Herceptin] and T-DM1, as it was an eligibility requirement, and about two-thirds also received pertuzumab [Perjeta]. These are what we would consider the most potent HER2- targeted therapies available today, and this study represents a modern cohort of patients treated with the best therapies for HER2-positive breast cancer who still have a need for more therapy.
Also, about half the patients on the trial were hormone receptor positive as well as HER2 positive, which is within range of what we typically see with HER2-positive disease. Ninety percent had visceral metastases— again, something we expect with HER2-positive breast cancer. And 13% had brain metastases. These are, of course, patients who had treated and stable brain metastases when they enrolled on the trial.
We enrolled patients from 3 continents on this study.
Can you discuss the efficacy data that led to the approval?
The primary end point of the safety trial [DESTINY-Breast01] was objective response rate as determined by independent review. In the trial of these heavily pretreated patients, we saw an overall confirmed response rate of 60%; this is consistent with results from the phase I study. It is always reassuring to have validation and consistency of data. Overall, the disease control rate was 97%, which means that almost every patient we treated with trastuzumab deruxtecan had some benefit.
As important in some respects is the durability of the response. There is a median duration of response of 15 months, so patients stay on this therapy for a really long time. The overall median progression-free survival on the trial was 16 months.
To put this into perspective, using the currently available therapies for refractory patients who are in the third-line setting and beyond, we would expect to see response rates of 10% to 30% and a median progression-free survival of 3 to 6 months. So the data for trastuzumab deruxtecan are striking. I think this is an extremely active treatment, and the phase II data are impressive in terms of the anticancer activity.
Can you describe the mechanism of action?
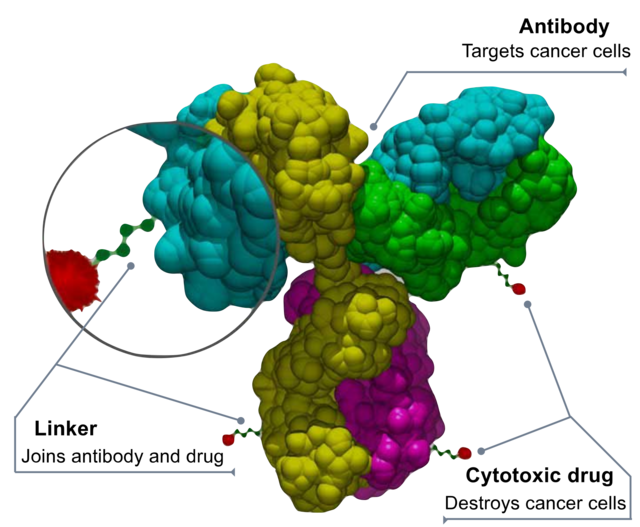
Trastuzumab deruxtecan is an antibody-drug conjugate; these are unique drugs designed to provide targeted delivery of very potent anticancer therapy. Trastuzumab deruxtecan is comprised of a HER2- targeting monoclonal antibody, essentially trastuzumab, and attached to this via cleavable linkers is a cytotoxic, also called the payload. In this case, that payload is deruxtecan, which is a topoisomerase I inhibitor.
We don't routinely use this type of chemotherapy agent in the treatment of patients with breast cancer, so not only is trastuzumab deruxtecan a very potent therapy, but it's also very novel. If we compare trastuzumab deruxtecan with T-DM1, which is the other available HER2-targeting antibody-drug conjugate, we see some notable differences. The payload for T-DM1 is a tubulin-targeting type of chemotherapy that patients with breast cancer are often already exposed to in other lines of therapy, so it is not as novel. Additionally, there are twice as many chemotherapy molecules linked to each antibody with the trastuzumab deruxtecan—approximately 8— compared with 3 to 4 with T-DM1.
The chemotherapy in trastuzumab deruxtecan also has a very short halflife and is membrane permeable, unlike the chemotherapy in T-DM1, which cannot permeate cell membranes. This allows trastuzumab deruxtecan to be active against not only HER2-positive cells but also surrounding tumor cells that may not have HER2 expression, hence a broader range of activity.
What else do we know about the agent's tolerability?
The most common adverse events that we saw on a day-to-day basis in the trial were gastrointestinal [GI] and hematologic which is what we might expect from a topoisomerase I inhibitor. The most common adverse event was nausea, which was managed successfully with antinausea medications. Overall GI adverse events were mild in nature and could be managed with supportive therapies. Bone marrow suppression leading to low blood cell counts were typically grade 1/2, and we were still able to deliver the therapy.
Lung toxicity is an important risk with trastuzumab deruxtecan that we first identified with this antibody-drug conjugate in the phase I study. We were vigilant for it in the phase II study. Overall, about 14% of patients in the phase II trial had some evidence of lung toxicity, and that ranged anywhere from asymptomatic findings on CT scans up to a few grade 5 fatal events from interstitial lung disease.
Potential lung toxicity is something that patients and physicians need to be made aware of because it requires careful monitoring of patient symptoms so that treatment can be interrupted, or sometimes even permanently discontinued, to prevent serious lung consequence. Education is going to be required when the drug is made available—educating the physicians who prescribe the drug as well as advising the patients to report any new or changing symptoms, particularly pulmonary-related symptoms, so that interventions can happen early and we can prevent serious toxicity.
On the other hand, we did not see concerning cardiac toxicity, which is a risk we do see with other HER2-targeting therapies.
How does trastuzumab deruxtecan fit into the current treatment paradigm?
Based on current guidelines for patients who have HER2-positive metastatic breast cancer, our preferred first-line therapy is a combination of a taxane chemotherapy plus trastuzumab and pertuzumab based on the survival data for this triplet therapy from the CLEOPATRA trial [NCT00567190]. In the second-line setting, we tend to use T-DM1 because it has proven to be superior to the other available options.
This leaves trastuzumab deruxtecan as a drug for the third-line setting and beyond.
What are the next steps for trastuzumab deruxtecan?
A number of phase III trials are already under way. First, the confirmatory phase III randomized trial for our DESTINY-Breast01 study, called DESTINYBreast02 [NCT03523585], has been open for over a year and is currently enrolling the same population of patients with HER2-positive metastatic breast cancer who have had prior T-DM1. Patients will be randomized to either trastuzumab deruxtecan or physician's choice [of capecitabine plus either trastuzumab or lapatinib].
Second, DESTINY-Breast03 [NCT03529110], another randomized phase III trial, is examining trastuzumab deruxtecan in the second-line setting. These patients will be randomized to either T-DM1 or trastuzumab deruxtecan, so it is a direct comparison.
Finally, the randomized phase III trial, DESTINY-Breast04 [NCT03734029], is enrolling patients with HER2–low breast cancer. In this study, patients who have HER2 1–positive or 2–positive (FISH negative) expressing breast cancer will be randomized to either trastuzumab deruxtecan or physician's choice of standard-of-care chemotherapy.
We know that trastuzumab deruxtecan is extremely potent, and in the early preclinical work, even HER2–low expressing cancers were susceptible to the effects of this antibody drug conjugate. The phase I trial of trastuzumab deruxtecan included a cohort of patients with HER2–low expressing breast cancers, and these patients also had a substantial response rate to trastuzumab deruxtecan. This is the first HER2 targeted therapy that seems to work in in cancer which we have traditionally called HER2 negative. It's very exciting to think we might be able to take advantage of targetinng HER2 for a whole new population of patients.
Trastuzumab deruxtecan is active not only in breast cancer, but also in HER2-expressing gastric cancers, and investigators are looking at it in colon cancer, in lung cancer, and in patients with other HER2-mutated cancers. It is active across a broad spectrum of tumor types, and studies are also looking at it in combination with other targeted therapies to maximize its potential.
At some point, we may be able to move this drug into an early stage setting, where the goal is to try to cure more patients and prevent recurrences.
Is there anything else you'd like to highlight about this drug?
In spite of the successes, there still remain areas of unmet need for patients with HER2-positive disease—specifically the treatment and prevention of brain metastases. This is an area where we need to study trastuzumab deruxtecan's efficacy specifically, and I know that preclinical studies and clinical studies are either under planning or under way in this regard. This past year we also saw data for other promising HER2-targeting therapies that could also be options for our patients one day. This keeps me optimistic about the future.
Editor's Note: This interview took place prior to the FDA approval of fam-trastuzumab deruxtecan-nxki for the treatment of adult patients with unresectable or metastatic HER2-positive breast cancer who have received ≥2 prior anti–HER2-based regimens in the metastatic setting.
1 -
There are numerous fascinating articles & videos on www.onclive.com describing the advantages to this relatively new drug, fam-Trastuzumab Deruxtecan, what we will be calling Enhertu.
It is well worth your while to go to the website & register (free) in order to access many, many articles that you will find helpful & informative.
Sometimes, I'll read an article 4 or 5 times in order to glean all the "stuff" out of it. It's great!
Here's a wonderfully encouraging video: https://www.youtube.com/watch?time_continue=4&v=IAZBvZYGzUM&feature=emb_logo
0 -
- Approved in Japan: https://www.onclive.com/web-exclusives/trastuzumab-deruxtecan-approved-in-japan-for-her2-metastatic-breast-cancer
Trastuzumab Deruxtecan Approved in Japan for HER2+ Metastatic Breast Cancer
Jason M. Broderick @jasoncologyPublished: Wednesday, Mar 25, 2020
 The Japanese Ministry of Health, Labor, and Welfare (MHLW) has approved trastuzumab deruxtecan (Enhertu) for the treatment of patients with HER2-positive unresectable or recurrent breast cancer who have had prior chemotherapy and are refractory or intolerant to standard treatments.
The Japanese Ministry of Health, Labor, and Welfare (MHLW) has approved trastuzumab deruxtecan (Enhertu) for the treatment of patients with HER2-positive unresectable or recurrent breast cancer who have had prior chemotherapy and are refractory or intolerant to standard treatments.
The approval is based on findings from the phase II DESTINY-Breast01 trial, in which the antibody-drug conjugate (ADC) trastuzumab deruxtecan induced a confirmed objective response rate (ORR) of 64.1% (107 of 167 evaluable patients; 95% CI, 56.3-71.3)."Our researchers in Japan have worked diligently on our ADC technology and we are excited to bring Enhertu, the first of many ADCs we have in development, to patients with HER2-positive metastatic breast cancer in Japan. Results seen with Enhertu are impressive as most women benefited from treatment with durable responses lasting a median duration of more than 14 months," Wataru Takasaki, PhD, corporate officer, head of Oncology Function and Head of R&D Division in Japan, Daiichi Sankyo, said in a press release.
The safety population evaluated by the MHLW included 184 patients, 182 (98.9%) of whom experienced at least 1 adverse event (AE). The most common AEs were nausea (76.1%), alopecia (46.2%), fatigue (44.0%), vomiting (42.4%), neutrophil count decreased (29.9%), decreased appetite (28.3%), anemia (21.7%) and diarrhea (21.7%). Interstitial lung disease (ILD) occurred in 8.2% of patients, but there were no grade ≥3 events.
In the United States the FDA granted an accelerated approval to fam-trastuzumab deruxtecan-nxki in December 2019 for the treatment of adult patients with unresectable or metastatic HER2-positive breast cancer who have received ≥2 prior anti–HER2-based regimens in the metastatic setting.
The available data from the phase II DESTINY-Breast01 trial at the time of the approval showed that trastuzumab deruxtecan induced a confirmed ORR of 60.3% (95% CI, 52.9-67.4) per independent central review (ICR), including a 4.3% complete response (CR) rate, and a 56% partial response (PR) rate.2 Sixty-seven patients had stable disease (SD; 36.4%), and 3 had progressive disease (PD; 1.6%). Two patients were not evaluable. ORRs were consistent across subgroups, including those with prior treatment with pertuzumab (Perjeta; 64%) and those with ≥ 3 prior regimens (59%).
In the open-label, international, multicenter phase II registration study, investigators enrolled 184 patients with HER2-positive breast cancer who were heavily pretreated, including with T-DM1 (Kadcyla) and other HER2-targeted treatments. The trial consisted of part 1 to evaluate pharmacokinetics (n= 65) and to determine recommended dose (RP2D; n = 54) for part 2 (n = 134): 5.4 mg/kg fam-trastuzumab deruxtecan-nxki. Data from this study were published simultaneously in the New England Journal of Medicine.3
ORR per ICR served as the primary endpoint. Secondary endpoints included DCR, DOR, and PFS.
Inclusion criteria included ≥18 years of age, unresectable and/or metastatic breast cancer, HER2-positive (centrally confirmed on archival tissue), prior T-DM1 therapy. Patients with a history of significant interstitial lung disease (ILD) were excluded. Those with stable, treated brain metastases were allowed.
All patients were female, the majority were white (55%), and 38% were Asian. Median age was 56 years (range, 28-96 years). Fifty-three percent were hormone receptor (HR)-positive and 45% were HR-negative. At baseline, the median number of prior treatment regimens was 6 (range, 2-27), including trastuzumab (Herceptin; 100%), T-DM1 (100%), pertuzumab (65.8%), and other HER2-targeted regimens (54.3%). The reported best response to T-DM1 before enrollment on the study were a CR and PR rate of 22%, 21% of patients with SD, and 36% with PD. Twenty-one percent were not evaluable.
As of the data cutoff (August 1, 2019), 79 patients (42.9%) are still on treatment, while 105 patients (57.1%) discontinued treatment, primarily for progressive disease (28.8%). In total, 184 patients enrolled on the study have received 5.4 mg/kg T-DXd for a median treatment duration of 6.9 months (range, 0.7-16 months).
Moreover, the investigational HER2-targeted antibody-drug conjugate yielded a median duration of response (DOR) of 14.8 months (95% CI, 13.8-16.9), and a disease control rate (DCR) of 97.3% (95% CI, 93.8-99.1). Clinical benefit ratio at 6 months was 76.1% (95% CI, 69.3%-82.1%), and median time to response was 1.6 months (95% CI, 1.4-2.6 months). Activity of fam-trastuzumab deruxtecan-nxki across all major subgroups appeared consistent.
After a median follow-up of 11.1 months (range, 0.7-19.9 months), median progression-free survival (PFS) of 16.4 months (95% CI, 12.7-NE). Median PFS in the 24 patients with brain metastases was 18.1 months (95% CI, 6.7-18.1 months). Median overall survival was not reached (95% CI, NE-NE).
For the approval, the FDA evaluated the safety of fam-trastuzumab deruxtecan-nxki in a pooled analysis of 234 patients in the DESTINY-Breast01 and Study DS8201-A-J101 trials.
Specifically, in DESTINY-Breast01, treatment-emergent AEs (TEAEs) occurred in 99% of patients, 51% being grade ≥ 3. The most common any-grade TEAEs were nausea (77%), alopecia (48%), fatigue (48%), vomiting (45%), constipation (34%), decreased neutrophil count (31%), decreased appetite (29%), diarrhea (27%), and anemia (26%). The most common grade ≥ 3 AEs were decreased neutrophil count (in 31% of the patients), nausea (7.6%), and anemia (in 26%).
Of note, 25 patients (13.6%) experienced ILD related to fam-trastuzumab deruxtecan-nxki by an independent adjudication committee. However, ILD was primarily grade 1 (2.7%) or 2 (8.2%). Median time to investigator-reported onset of ILD was 193 days (range, 42-535 days), and 13 of the 20 patients with grade ≥2 ILD received corticosteroids. Overall, 7 patients recovered, 2 were recovering at data cutoff, 12 were either outcome unknown or not followed until resolution, and 4 died. Of the 4 fatal cases, onset was from 63 to 148 days, of which 3 received steroids as part of their treatment, and death occurred 9 to 60 days after ILD diagnosis.0


