NEW Oncotype Dx Roll Call Thread
Comments
-
Oncotype score of 29 here, with an 18% recurrence rate, so my treatment plan moved from lumpectomy and radiation to lumpectomy, chemo, then radiation. Starting a CMF regime on Friday, November 1st.
0 -
Hello to all...
Found out yesterday my Oncotype RS is 18. I have ILC the tumor currently measures 7 cm x 10 cm. And there is pectoral muscle involvement.
The first MO said Endocrine Therapy only as Chemotherapy and Radiation would not be effective.
The second MO has recommended (3) 28 day cycles of CMF. Then another MRI before MX. Then after the Pathology report after Surgery then the decision regarding Radiation will be decided. AIs for 10 years after that.
I have not done well on AIs in the past. I have Rheumatoid Arthritis and the SEs were unbearable. I'm hoping new things have been developed to cope.
Bone Scans and CT Scan were clear but I'm told the Breast MRI is the definitive test for muscle involvement.
8 years ago my chance of recurrence for IDC Breast Cancer was considered to be 5% after treatment. I guess they were right, it's a different type now.
The conversation yesterday included the word “Cure." I'm told the word simply means that I'm probably going to die from something else before the Breast Cancer kills me. 🥴
I suppose that's one way to think about it.
Living is good
0 -
Hi,
I posted before that I requested oncotype myself since I don't have other insurance, and our basic insurance provided by government does not fund this test. Today, I went for my first meet with radiologist, and I will see MO again this Wednesday for my oncotype score. To my surprise, the radiologist said, based on my score, they think the MO won't recommend chemo for me, so they just plan my radiation based on this. They plan 20 radiation for me, and supposed to start in two or three weeks. If I will do chemo after discussion with MO this Wednesday, I shall call them to let them re-schedule my treatment plan, of course MO office will also notify them.
So now comes the question, to which score (they do mention I am low risk) and to which percentage of chemo benefit, MO won't recommend chemo? I hate they don't tell me the score right there, I called MO office around ten days ago, they already got the score but just cannot tell me, and no way to have an earlier appointment.
0 -
hello Cathy, Please post your onco score when you receive it. Sounds like it will be low. Why couldn't the RO give you your score?? Generally, if your score is under 25, they would not recommend chemo. My score was 48 with a recurrence rate of 37% with AI alone, so I did chemo. But, scores and recurrence rates are not always consistent. I know of someone with a higher onco score than me with a recurrence rate of 32% . I had a grade 3 tumor, so that probably played into my higher recurrence percentage. Best of luck to you, no matter what you decide. Keep us posted. Pat👍
0 -
Hi UpstateNYer,
Mine is node positive case, so the cut-off policy is different. Actually the corresponding clinical trial has not been finished yet, the latest nccn guideline mentions something but without firm statistics. It mentions score 11 and score 18, don't know where is the cut-off for low risk. So my plan is, opt no if under 11, opt yes for dd ACT if over 18, op yes for TC is between 11 and 18. I think, it shall be under 18, since radiologist said it is low score, but not intermediate.
I will post here.
0 -
Hi Cathy67 - mine was also a node positive case and at an Oncotype of 21, the results were that chemo would provide zero benefit for me vs tamoxifen. So my oncologist said he would not recommend chemo “due to the extra toxicity it would introduce for no benefit”.
Yes he used the word “toxicity” and this is a doctor who regularly treats patients with chemo. Your Oncotype score should show a % risk of recurrence with tamoxifen alone vs tamoxifen plus chemo and you should weigh the benefit of chemo vs the risks.
The risks of chemo can be very real. While there are many examples of people - many on this board - who fare through chemo just fine, keep in mind there are serious risks before you sign up for it. Permanent neuropathy is a common side effect. My friend just posted about her friend who is now in hospice care as a result of chemo to fight breast cancer. If your MO is not recommending chemo, that’s a good thing. I don’t know why they aren’t telling you your score, I think you have a right to ask for it. My MO shared the entire test with me and I got a copy to keep for myself.
Anyways, all our cases are different, but I wanted to let you know of mine because I was also node positive, did not require chemo, did do radiation and am taking tamoxifen, and also just had a completely clear and cancer free mammogram! And I’m faring really well, have been able to still feel like me through this entire journey, got through this past year with very few side effects.
Best of luck to you and whatever you decide I support. Just want to help you be as informed as you can before you make an important decision on your treatment plan!1 -
Hi PebblesV,
The rule here, only MO can talk with that report with me, after that, I can get copy of the report from any office. MO's appointment is so hard to make, it will be tomorrow.
Thanks for the info, it is so useful! However, I wonder why score 21 give you almost zero chemo benefit? I assume score increases as recurrence risk increases and chemo benefit increases as well. Having low chemo benefit means low recurrence rate which is great, though one may face hard decision. Before my test, MO said, he has seen so many cases happened at my situation, so he insisted dd ACT, but not TC 4 rounds. I've studied nccn guideline, for node positive, the corresponding clinical trial has not been finished, nccn said, it has not been decided which score is the cutoff for low risk, score 11 vs. score 18....However for node negative, it already has clear recommendation.
I wonder maybe your two nodes are under 2mm, so they put your case as node negative? I don't know if micromets be in node negative or node positive group.
Thanks!
0 -
Hi Cathy,
Glad it's helpful! The Oncotype report provides a % risk of recurrence with tamoxifen alone and a % risk of recurrence with tamoxifen plus chemo. In my case that % was exactly the same (I think it was something like 13%) in both scenarios. That's why it will be so great for you to look at your own report!
Also the Oncotype is based on 21 genes they measure in the tumor and the report gives a measure of how far you are on the PR and ER + and HER2 - scale. In my case I was very PR/ER positive which I think is another reason it came out as tamoxifen being just as effective as chemo. These are all things you should be able to see when you view your report.
I AM on tamoxifen FYI. I've been tolerating it well luckily and in a way I feel it was my ticket out of chemo so I should take it.
I just think if your docs are not insisting on chemo for you, that's a good thing. Chemo is brutal. I've seen too many people on a personal level go through it and lose themselves. There is also someone on the threads (Meoww) who had an oncotype score of 34 and refused chemo even though in her case it was recommended and she is 6 years (maybe 7 now) out NED now. You just have to make a really informed decision on the treatment you are willing to do for what benefit you get and what risk you are willing to tolerate. Best of luck and keep us posted
0 -
Hi PebblesV,
Sounds I already got cancer brain! I know what brings me this misunderstanding!!
You mentioned oncotype 21 which is the test name, I misread it as oncotype score is 21, then I have the question why score 21 turns out zero chemo benefit.
Thanks for the patience, I am really too too nervous in the past month, I've included depression drugs in my question to MO.
0 -
Hi Cathy,
You read correctly, I had an Oncotype score of 21, and the test reviews 21 or 22 genes in the tumor. For me, the score of 21 with a node positive case meant zero chemo benefit. It said that my risk of recurrence was 13% of I took tamoxifen and 13% if I did tamoxifen plus chemo. So, no difference in % risk of recurrence with chemo, and therefore no chemo.
Totally, totally understand the nervousness. Honestly for me, the waiting for results and a plan was the hardest part and caused me a lot of anxiety as well. Once I had all my results and an agreed-upon plan of action that I felt good about and my doctors were aligned with, it was ironically a lot easier, even though I had to go through treatment. So I get it!
These might be some helpful articles re: interpreting Oncotype DX scores. I also think it will make a lot more sense to you once you can see your report.
0 -
Cathy, here are two graphs I've found on-line that show how Oncotype scores line up with 5 year risk for Tamox alone vs. Tamoxifen +chemo, for Node Positive patients:
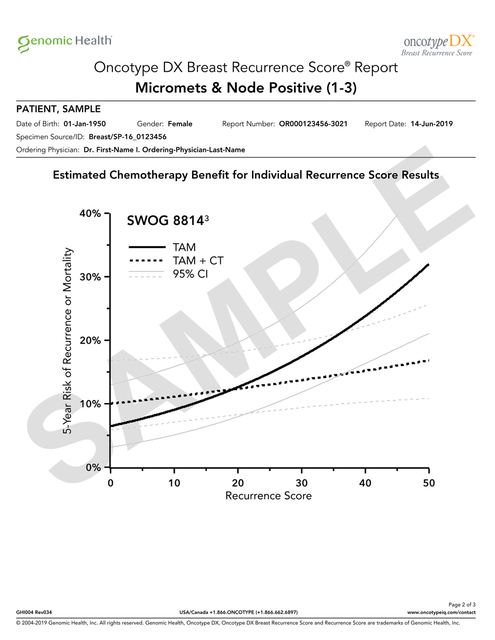

Both graphs represent results from the same study but the second breaks the results out by number of positive nodes. The top graph appears to be current - it states "2004-2019" on the bottom. The second chart is older - it states "2004-2010" on the bottom. So my guess is that if your report includes a graph, it may be the same as the top chart here.
0 -
Beesie,
Thanks!
Did I mention that my radiologist said, he thought MO won't recommend chemo based on my oncotype score (but nobody told me due to the policy in BC)? I will meet MO tomorrow late afternoon, if no chemo is the final decision, can I ask msp to fund me this test fee? $4380.00, cause I saved chemo fee. If my node is 1mm less, then I won't need to pay this huge amount of money. Of course, if it turns out low risk and no chemo, this amount of money is definitely worth to pay.
Will get back here. Breast cancer kills all my time for study.
0 -
Hi,
I just got my oncotype score, it is 6 with 11% as 9 year recurrence rate with AI only, so no chemo!
The report only has two pages, just like the sample report on their website, however on the sample report, score 10 with 12% as 9 year recurrence rate, sounds score difference does not influence recurrence rate difference a lot.
Just as MO said, since I order the test, I shall trust it, otherwise I shall not order it. So I trust it, and I wish technology will move forward quickly, so even someone it happens, we have more ways to deal with it.
Thanks ladies!
0 -
hello Cathy, So happy that your Onco score is so low. Such great news. Will you be doing rads? When will they start? Wishing you all the best. Pat
0 -
Pat,
Thank you! Yes, I will start radiation later this month, will have 20 rounds.
Also I will do that injection every three months, and start to take AI after radiation.
Great to skip chemo!
0 -
Cathy, Is the injection you're speaking about for your bone density? You should do fine with rads. Much, much easier than chemo. I did not experience any nausea or fatigue with rads. I only needed 16 txts, as I had IORT during first lumpectomy. Best wishes. Pat
0 -
Hi Pat,
It shall be lupron injection to ovaries, and then arimidex. My ER is 10.2 compared to 8 out of 8 in biopsy report, and PR is 9.3 compared to 5 out of 8 in biopsy report, PR is actually very strong and HER2 is 9.3.
0 -
hi Cathy, I am doing great so far on Arimidex. Been taking it since Sept. 5th. Hoping to not experience joint pain, mood swings, etc. I started it before rads started, as I was diagnosed in early Feb. MO said I could wait until after rads to start arimidex, but I wanted to start it asap. Hoping the Lupron injections go well for you too. Take care. Pat👍
0 -
Hi Pat,
How is lupron injection? Is it painful?
Do I need friend to ride me back? It is only 30 minutes walk to hospital.
0 -
hi Cathy, I never had Lupton injections. Sorry if my previous post was not clear, instead of "too", I should have said " as well". Perhaps if you go under " search" on this site, you will find guidance from others who have had it. Hope it goes well for you. Pat
0 -
Cathy - congrats on the low oncotype score and no chemo! Like upstateNY, rads was pretty easy for me to tolerate too. Look up Miaderm to avoid radiation burns (it’s on Amazon).
Agree it seems like the score varies more than the recurrence rate. Yours is 6 with 11% recurrence and mine 21 with 13% recurrence
0 -
Hi everyone,
My Onctotype is 15 and I am premenopausal at 54, so I think I should be evaluated as under 50. They are recommending radiation due to lymphovascular invasion. My MO was unsure on chemo so sent me for second opinion. She say, NO chemo, because chemo doesn't work that well on ILC and miotic=1. They thought I would be happy, but I'm scared not doing it. As discussed above, the node positive results are not as conclusive as node negative, NCCN is still not definitive pending rxponder study 2022, I have lymphovascular invasion and extranodal extension. When they don't do ALND, you could have more nodes positive that we are not aware of. He agreed I should get another opinion. I'm also nervous to keep dragging this out, but I can't find peace with this decision. I've wanted to go to Sloan all along, so that is my next step. Have an appointment 11/18. I am a huge skeptic of limited data studies. For example, the node negative under 50 group shows I would get some benefit, but the node positive report doesn't. Also, they lump things together. The SEER registry data is skewed because it includes micromets with 3 positive nodes. Than they found for some people that stop endocrine therapy at 5 years, they see a recurrence. Is the endocrine therapy just making the cancer lie dormant so it can come back in the distant future? or does it die if it can't grow? I can't find peace with this!!!
0 -
Yeah, you are at gray area. I am 52 years old, last period is six months ago, they also treat me as premenopausal. Mine is 6, so easier to decide. On report, they put under 17 as low disk. My backup plan is to ask for TC 4 rounds, if I get 11 to 17, but it turns out 6, so MO and RO all say no chemo.
Hugs, I know it is not easy.
0 -
Hi JRNJ,
You can find in the latest NCCN guideline, they mention low risk cutoff score, score 11 vs. score 18, don't know at this moment. From my study, I think score 15 is the gray area. Sorry that you got it.
How many percentage of 9 years remote recurrence on your report? On mine, it is 11%.
And my ER is 10.2 (8 out of 8 in my biopsy), PR is 9.3 (5 out of 8 in my biopsy) and HER2 is 9,3 (0 out of 3 in my biopsy).
0 -
JRNJ - I wanted to provide you some reassurance on the no chemo and no ALND path for you. I was also node positive, no chemo, no ALND and just recently had a mammogram that came back clear and cancer free! Oh and I’m premenopausal too at 44. A few things having gone through this that I hope can reassure you:
(1) Radiation can still treat the nodes just in case. I went through radiation and my radiologist told me he treated the nodes too. There is a much lower risk of lymphedema with radiation vs ALND (15% vs 40%).
(2) There are studies showing that 30 min of exercise 5 days a week can reduce your risk of recurrence by half, so there are things you can do beyond treatment to keep the cancer from coming back.
(3) You can also still treat the nodes and any other possible place cancer might pop up with hormone therapy (usually tamoxifen for premenopausal) which has been shown to be more effective as or just as effective as chemo for lower oncotype scores. So it’s not like you aren’t treating it if you don’t do chemo - you are treating it, just with radiation and tamoxifen that generally have less severe side effects than chemo.
If your doctors are saying you do not need chemo, you are very fortunate and I feel in a position to beat this with less worry on side effects from treatment. I am currently reeling from a personal story a friend shared re: her friend who had learned she had breast cancer last July, went through chemo, and is suddenly in end of life hospice care. These are the stories that don’t get shared and it’s heartbreaking and was due to SEs from chemo. I have sadly witnessed firsthand how brutal chemo can be, this also took my mother-in-law. And I remember when this all started for me and I thought I might need chemo and I met a group of survivors I thought would help me feel OK about it, and this lady introduced herself saying, “Sorry if I don’t remember your name but chemo destroyed my brain cells.” And I asked if she finished it very recently thinking this was a temporary SE and it would all bounce back and she said no, it was 15 years ago and if she knew then what she knew now she wouldn’t do it.
So, I think if your doctors are saying you don’t need chemo, that’s a good thing and there are lots of things from other treatments to what you can do personally to prevent a risk a recurrence.
I should caveat that for those who do need chemo and do it, I’ve seen plenty of cases as well where people get through just fine and come out the other end. And I understand the cases where there really is benefit, then the risk/benefit scenario makes more sense. But in the case where the benefit isn’t there, don’t chase after something that could be more harmful than beneficial.0 -
Thanks PebblesV,
When we decide whether chemo or not, we look at absolute chemo benefit. For me, report says no absolute benefit. Just as my MO said, since you ordered the test, then you shall trust it, otherwise why you ordered. So, I trust oncotype, I opted no to chemo, my MO and RO all say no to chemo. Sometimes, we may hear the cases of recurrence, oncotype predicts absolute chemo benefit to help for chemo decision, it also predicts the distant recurrence rate, looking at the rate, for node positive, it is a bit above 10%, mine is 11%, no surprise some recurrence cases among no chemo groups, however, same thing happens among chemo groups, there is no significant difference between those two. Oncotype provides those clinical trails on the report, you can find details on internet I don't know what will happen in the future after my treatment, what I can refer today, only the technologies and those finished clinical trails. In one world, I trust chemo benefit, and pray I won't fall into the 11% group, it does not matter whether chemo or not.
0 -
Thanks for the input.
Cathy, yes, I have the NCCN guidelines. I don't understand why you and I read it, but none of my doctors, lol. My recurrence is 14%. My biomarkers are expressed as %, ER 99, PR 100, Ki67 18 HER2 0 from a biopsy. Previous biopsy was ER 70, PR 90, Ki67 10 HER2 Neg. I questioned the discrepancy and one Dr. said close enough to be good. They didn't test the final pathology because they said it had already been done twice on the biopsies.
I know I should be glad to not do chemo. I have an uncontrollable fear that the cancer is spread more then they know already. I have weird pains in my arm and side. I have an uncontrollable fear that we won't get it all without chemo. I'm not worried about 3 years or even 7 years, I'm worried about 15, 20. ILC is slow growing and comes back later. But I'm slowly getting there. I think I will have closure after meeting with Sloan.
Pebbles, Sorry to hear about your friend. Do you know what type of chemo she was on? If I did chemo, it would be 4 treatments of T and C.
Judy
0 -
Hi Judy,
So your doctor recommended TC 4 rounds? This is the easiest regimen. Before my oncotype test, my MO recommended dd ACT 8 rounds with 5% estimated absolute chemo benefit, I asked for TC 4 rounds, he said TC does not work for me due to my one positive node. Then, I ordered oncotype test, I am in Canada, our insurance does not cover over 2mm deposit, mine is 3mm, I paid CA$4100 for that!
And our biopsy report does not have ki67.
So you don't have confidence to skip chemo, if so, how about you research TC 4 rounds, I know it is doable. if I were at your situation, my plan is TC 4 rounds. My plan is no chemo if under 10, TC 4 rounds if 11 to 17, dd ACT if over 18.
0 -
cathy67, I did TC x 4. It certainly was not easy. It was very, very difficult for me. The first 2 txts. gave me horrible side effects. I had a migraine headache and nausea for a week after first one, nausea and body aches for a week after the second txt. , not to mention the horrible fatigue the whole time. I have pain in my shoulder area that has not gone away post chemo. I was going to stop txt. after the second one, but at my request, MO increased iv fluids and decreased chemo by 10% for 3rd and 4th txts. It made it at least bearable. So to those of you that do not need chemo of any kind, be very grateful.
0 -
UpstateNYer - thank you for being so candid about your experience and kudos to you for getting through chemo. I'm glad it's in the past for you and sendingyou well wishes on the next stage of your journey.
Judy - I don't know the details of my friend's friend's chemo and unfortunately cannot pry or ask now. I agree with UpstateNYer that it's a blessing you do nothave to do chemo. I was hoping my experience could provide you with the details and reassurance that you can successfully come out of this cancer free with the treatment your docs are recommending, and that radiation and tamoxifen do treat “stray cancer cells" and will map the path for radiation for node positive patients to treat the nodes. You need to do what feels right for you, just make sure it's an informed decision with details on your own risk/benefit scenario and what risk you are willing to take for what benefit. Make sure you understand all the SEs and % risk before you undergo something, and if you're OK with that % risk for the % benefit you are going to get, that's great, move forward with confidence. If you're not OK with the % risk for the % benefit, that's also fine, and walk down the other path with confidence.
Hope that makes sense. The details I shared were just to help you be informed. And ideally reassured by another node positive case.In my case, once my results came back that showed the same exact % risk of recurrence with or without chemo, my MO actually said he “would not introduce the added toxicity of chemo to my system for no benefit". It just always stuck with me that my MO who treats many bc patients with chemo, and successfully, still described it as a toxic thing to your system.
0