oncotype scores..
Comments
-
my Magee caculates to around 17.
Even if I put in the lowest possible grade 3/9, 300 each for Er/Pr, and 1 ki67, it only gets down to around a 7 for my 1.1 cm tumor. There must be something else that comes up with the ultra low oncotype score.
0 -
The Magee formula is a very simplified version of the Oncotype score. The Oncotype score has 16 inputs and 5 reference genes. Some are unfavorable factors that serve to increase the score, while others are favorable and decrease the score.
I posted this earlier in this thread:
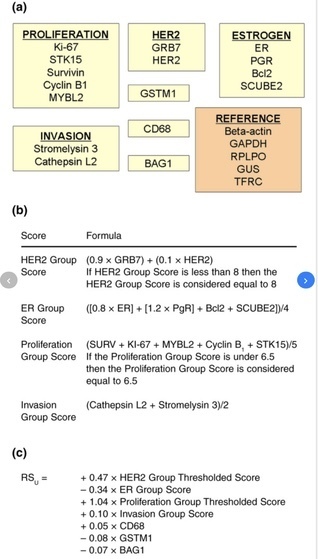
farmerlucy, your cancer cells may have had a really strong presence of GDTM1 and BAG1, whatever they are. Or maybe a high Bcl2 or SCUBE2. Those are the genes that lower the score, in addition to having high ER and high PR.
Yeah, I'm thinking it was the SCUBE2.
 0
0 -
When I do the equation the average is 20 . My Onco score was 31. Go figure I guess. Even before the Oncotype test results came back - when my MO saw I had the BRCA2 mutation (tested before surgery to determine treatment plan) and a Ki-67 of 60 (biopsy) she considered me to be at a high risk of recurrence. I did read that if you have a high Ki-67 but also have a high ER AND PR it's not very determinant. I had like 100% ER and 95% PR, so there is that. Thanks for posting the equation. Since it gave me a significantly lower score than the Oncotype, I like that test LOL
0 -
Yes, 51.🍀
0 -
I've used the equation according to my path report results and I get around 28. My oncotype was 51. Any idea why there would be such a discrepancy. My onco report had lower er and pr but not significantly. Thanks.
0 -
Emily, do you mean that the Magee calculation was wrong as compared to your Oncotype result?
To my post July 29 2020 post above, the Magee formula is a very abbreviated version of the Oncotype test. It provides a close approximation to the Oncotype score in most cases but not all cases. Your cancer cells might have a high presence of some of the more obscure (to us) factors in the Proliferation and Invasion groups, thereby driving up your score. Also, since your HER2 was negative on FISH, that likely means it was equivocal on IHC testing, so your cancer does have some HER2 presence, which could count in the Oncotype score. If the GRB7 is high, that could also be a big factor to drive up the score.
0 -
Thanks Beesie, my pathology was very ordinary, trying to get my head around 51 oncotype score. Its like an itch I keep scratching. Treatment is done and I'm OK, but as a Histology scientist I can't drop it. 😂I'll have to give it up I'm going Google eyed reading small print. X Anne
0 -
my oncotype score was 0...is that even possible? Did I really have cancer
0 -
I seem to recall one other person who had a 0 Oncotype score. I think it's possible because the formula (see my post above) includes both pluses and minuses that are summed together to get a total. So if the genetics of your cancer cells include a lot of favorable factors, they could cancel out the unfavorable factors. Just guessing, but I suppose it's possible that the sum of all the variables might even come out as a negative number, which probably would be bumped up to zero.
Well, the good news is that there's no question that you would not benefit from chemo!
0 -
Thanks Beezie, definitely no chemo...only Anastrozole for 5 years
0 -
just reviving this, I don’t have the K score and trying to guess the H scores with >66 staining strongly for Er and PR, so hoping this is somewhat accurate as I get a 19
0

