oncotype scores..
Comments
-
Sugar - Praying for you. I went through this almost 2 years ago. Luckily, I did radiation only and on Tam right now.
0 -
Mouse, I have no idea how to interpret. My score was 12, but 3% 9 years with Tamoxifen. Yours was 4 with a much higher score? Weird. I asked so many questions today, they said that were confident. Ugh
0 -
Hi Badluckbday
I had micromets in my lymph node - which put me on a different prediction table if you had nothing in your lymph nodes. Micromets mean its microscopic but still there. All the predictions are based on research and it keeps evolving - the micromets used to not even be detected.
0 -
Interesting. My oncologist ordered the BCI for no nodes and my score was 12. ( 9% recurrence rate ). However, it was later discovered that my ITCs were actually micromets. Now, I am wondering what my recurrence % would have been with the other test. There seems to be a big discrepancy between the 2 tests, based on the scores reported here. Oh well, I am almost five years out and scored high on the BCI so I guess it is a moot point now. All of this information changes fairly rapidly with new tests coming out and new study results coming in.0
-
Mouse, is there any way you could share the graph you mentioned? Or see if it tells you the % for a score of 12? Just curious how it compares to what I thought was my % for the last almost 5 years. 😀0
-
This is the graph = it is for micromets and 1-3 nodes positive - if I interpret it correctly, the lower scores do worse with CT - however, it is based on large database of (mostly) women and there may have been clinical reasons outside the oncotype score to recommend chemotherapy for some with low oncotype scores Also its tamoxfen results which don;t apply to me since I am post menopausal and will do AI
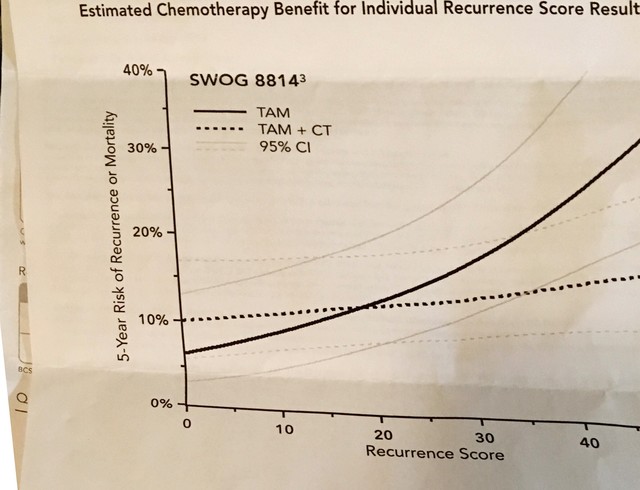 Also its0
Also its0 -
Thanks, Mouse! It looks like it is only 2 or 3 % points between the tests.0
-
Wow, you are knowledgeable. I wanted to pick your brain. My Mammaprint was ordered kind of as a side thought by my BS at 4 weeks postop. It was done on surgical bx. And results were high risk and luminal B. Shocked. Initial bx from core needle vacuum was grade 1 (tubule was 3 and others each 1), ki67 8%, idc with some dcis, 6mm, 99% estrogen and 80+%progesterone. Followup MRI was read by experienced radiologist and only knew where to look for tumor b/c of marker. USs x2 prior for wire placement and sentinel node did not show any growth. Bilateral reduction (large partial mastectomy with reduction on both sides) was negative for margins, tissue, and sentinel nodes. But path report said 9mm. I have upcoming appt with MO. I thought abt asking for new test. But what? And you are so right — the rep is who to talk to abt results. Very confusing since front page results are basically an aggregate for all high. I am discordant low clinical and high mammaprint with much better numbers. Thanks
0 -
My Oncotype score is 30. The oncologist is recommending chemo - four rounds of TC. He said I'm on the cusp of high so chemo is my decision but I value his opinion and will very likely go ahead with it. Just wrapping my head around it. I did TC 10 years ago so I know what to expect. As I always say...it's no picnic but it's doable.
0 -
Sugar, I'm now 2 infusions done out of 4 planned, dose-dense TC with Neulasta. Did you have Neulasta years ago when you had TC? My side effects from Round 2 so far aren't as bad as the first round. Some S.E. from the steroid. Best Wishes to you and to everyone here for a serene weekend. I had not been looking forward to my 68th birthday coming up in March, but now I am getting in the mood to celebrate.
 0
0 -
Hi Sweettalker - yes, I had Neulasta at each round of TC last night. Good luck with your last two treatments.
0 -
Thanks, Sugar77. How did you do with Neulasta side effects this time? Wishing you the best...
0 -
Sweettalker - I did fine with the Neulasta. I remember taking part in a bone pain study and had next to no issues. I took Claritin for five days with each shot and I think it helped.
0 -
Hello All,
Does anyone know if you have to get the Oncotype test done before you start your hormone therapy? I have read that a couple of places but I don't see it on the Oncotype website. Do you know if you have the Oncotype done after your start your hormone therapy, does it impact the results? If so, what are the impacts?
0 -
Thought I would share...
Waiting for my Oncotype score was stressful. I found Magee Equation. I am unable to post a link at this time but if you search for it and add Oncotype score, it will pop up
By putting in my specific information, the Magee Equation results stated my Oncotype score would be 17.89.
When my Oncotype score came in, it was 18. The Magee Equation was spot on. Thought someone might find a bit of peace using it, as I did.
1 -
Here's the link to the Magee Equation: https://path.upmc.edu/onlineTools/MageeEquations.html
It would be interesting to hear if other people find it to be accurate as well.
0 -
My equation score was 26, translating to an intermediate Oncotype score which was not my case. I think there may be exceptions due to type of mutation predisposing one to their BC.
0 -
I put in my information in the Magee Equation and got a 12.8. My oncotype was a 13, so pretty accurate in my case. My original pathology showed the Her2 to be equivocal, and if I used Her2 equivocal instead of negative, it gave me a score of 14.2.
0 -
Morning all, magee 25.5, oncotype 27 so pretty close . It also seems , in general, that ki67 and oncotype scores tend to be in really close proximity. There was a thread on that not too long ago and I found that interesting. Always exceptions of course
0 -
My Oncotype RS was 32% with 22% 10 year risk, the RSCP had a 6% 10year risk!! The Magee average score was 13.21748!
LT Lumpectory 9/16 7mm pure mucinous, 95% strong ER, 95% strong PR. Hr2- neg lymph
Radiation
Arimidex 2 years
Susan
0 -
How do I calculate the estrogen and progesterone boxes in the Magee equation? My ER was 98%, PR was 47%. I have the rest of the information. I really want to know......thank you
0 -
My Oncotype score was around at 16, as I recall, for my first cancer. As a part of the TailoRx trial, I was selected to get chemo. I had four rounds of Taxotere and Cytoxin. No radiation. 5 years of Tamoxifen and Arimidex. I was actually glad to get the chemo, as I wanted to throw everything at this disease. 12 years later, I was diagnosed with mets. We just never know.
0 -
Kksmom3, the H score should be listed on your original path report. There are formulas to calculate it, but you have to know how many cells stained strongly positive and how many cells stained weakly positive, as well as how many cells were negative.
0 -
It just said that the staining was "strong." That's probably not good, I assume? Just got percentage of Er -98% and PR - 47%. HER 2 neg. A member on here did private message me the formula, which I very much appreciate. I wouldn't have been a candidate for an Oncotype and wasn't, since, thankfully, I had DCIS with 3mm of IDC thrown in......but I was curious if I'd had an Oncotype, what might my score have been. Here's the kicker -my Ki-67was 37%. That's what scares me. I had really good clean margins, no node involvement, but......you know.
0 -
kksmom3, I guess you could try the formula and assume that every cell that was positive was strongly positive. That might get you a ballpark anyway. If your ki-67 was that high I have a feeling your oncotype would be on the high side as well.
0 -
I didn't get an Oncotype as it was a 3 mm tumor found by accident in DCIS. I've read that oncotyping isn't necessary if a tumor is 5mm and under. I think I even read it on the Oncotype site. I've also read, although I can't find it, that a healing biopsy site might show a higher Ki-67, due to tissue healing. Makes sense but I can't find that or any info pertaiing to that. At any rate, I'm almost two years out, so it's all a moot point anyway. Thank you for your reply,
0 -
The reason that an Oncotype test is not recommended for such small tumors is because little to no testing has been done on tumors of that size. To my understanding, the smallest tumors in the TAILORx study were T1b, which is >5mm but <10mm. So the Oncotype results simply can't be applied with any degree of certainty to tumors that are 5mm or smaller.
While high Ki-67 generally translates to a higher Oncotype score, this is not always the case.
kksmom, with the information you've provided, and making some guesses (with varying degrees of conservativeness), I've played with some numbers in order to complete the Magee formula.
First is a mildly conservative estimate:
- Nottingham score - Grade 2 is either 6 or 7 so I input 7.
- ER H-Score - Being 98% ER+ with strong staining would probably put you almost at the full 300; 98% of 300 is 294. But to be conservative, I input 250.
- PR H-Score - Being 47% PR+ with strong staining would probably put you at about 50% of the 300; 47% of 300 is 141. But to be conservative, I input 100.
- Tumor Size - 0.3cm
- Ki-67 - 37%
- Equation 1 Result 22.56291
- Equation 2 Result 22.76811
- Equation 3 Result 22.88175
- Average Magee Equation Score 22.73759
.
Second is a more optimistic estimate (but still a bit conservative):
- Nottingham score - Grade 2 is either 6 or 7; I input 6.
- ER H-Score - Being 98% ER+ with strong staining would probably put you almost at the full 300; 98% of 300 is 294. I input 280.
- PR H-Score - Being 47% PR+ with strong staining would probably put you at about 50% of the 300; 47% of 300 is 141. I input 125.
- Tumor Size - 0.3cm
- Ki-67 - 37%
- Equation 1 Result 19.84896
- Equation 2 Result 18.53593
- Equation 3 Result 21.50765
- Average Magee Equation Score 19.96418
.
Last is what I think would be a very conservative estimate:
- Nottingham score - Grade 2 is either 6 or 7 so I input 7.
- ER H-Score - Being 98% ER+ with strong staining would probably put you almost at the full 300; 98% of 300 is 294. But to be very conservative, I input 150.
- PR H-Score - Being 47% PR+ with strong staining would probably put you at about 50% of the 300; 47% of 300 is 141. But to be very conservative and since PR is sometimes calculated to be lower using the Oncotype methodology, I input 50.
- Tumor Size - 0.3cm
- Ki-67 - 37%
- Equation 1 Result 25.94941
- Equation 2 Result 28.04961
- Equation 3 Result 26.50075
- Average Magee Equation Score 26.83326
.
Of course none of these are the same as having an Oncotype result, and it's all speculation. But based on previous comments, it appears that the Magee Equation is often quite close, so it's probably safe to assume that your results would be somewhere in the range of these 3 results, or at least not likely to be significantly higher.
0 -
Thank you, Beesie, for such an informative post. My Nottingham was a 6. When I did the calculation I got a 19 something, but your calculations make sense. Hoping I would have been between 19 and 22. I'll tell you if this aggressive little sucker had grown............ well, early detection is early detection!!! The mitosis score in the Nottingham was a 1. This did puzzle my oncologist a bit, but she didn't act like I should worry about it at all. Not like it would do any good anyway. So, I ty not to,,,,,easier said than done. I asked her if I was Luminal A or B, she said most certainly luminal A. Of course, this pathology is all after the lumpectomy. I asked her if I should have had a mastectomy. She emphatically said no. I know lump/rads - mastectomy are about the same risk of recurrence. I just gotta go with what's been done. Hopefully, it's gone for good!
0 -
A mitosis of 1 is great! It's inconsistent with the 37% Ki-67, which is probably why your oncologist was puzzled.
Here's the thing... a lots of cancer hospitals, including mine, which is the top treatment center in Canada and one of the top 5 cancer research centers in the world, don't look at Ki-67 because they feel that it is unreliable. I know for example that in the past MSK didn't test for Ki-67 although I don't know if that's still true today. Lots of patients, and their MOs, never know their Ki-67. I'm one of them. Like you, I had a mitosis score of 1, and my MO put as much emphasis on that as on the total grade, which was grade 2.
As for MX vs. lumpectomy, keep in mind that the Oncotype score and everything we are discussing here relates specifically to metastatic risk, the risk of distant (outside of the breast) recurrence. In most cases that die was cast well before the patient even knew that she had breast cancer - either some cancer cells slipped out and escaped the breast while the cancer was sitting there in the breast, or they didn't. And that's why the type of surgery done on the breast generally has no impact on the risk of recurrence beyond the breast.
It appears that most everything looks to be in your favor, with the mitosis score of 1, the high ER and the tiny size of your tumor. No matter how good the diagnosis, everyone who's had invasive breast cancer has some risk of mets. There are always things you can do to reduce that risk, but every treatment comes with it's own risks and side effects, and sometimes adding a treatment actually puts the patient at an overall greater health risk. This is exactly why chemo is not recommended for small tumors that are not high risk. Your tumor is definitely not high risk, so from that standpoint, it appears that you had the optimal treatment plan for your breast cancer and overall health.
0 -
Beesie, thank you so much for chiming in on this. I wish I hadn't even known the Ki-67 score, but my oncologist emphasized everything you just said. I'm a year and a half on letrozole and doing well on it. I can tell I have no estrogen by now, my skin is dry, and so is my nether region, but I can live with those side effects, as long as I keep on top of moisturizing everything, I'm ok. The letrozole should help my low recurrence rate as well.
I can't thank you enough for this explanation! You really eased my mind! I hope you are doing well! Stay safe during this stinking pandemic!
0



