Breaking Research News from sources other than Breastcancer.org
Comments
-
FDA grants accelerated approval to pembrolizumab for locally recurrent unresectable or metastatic triple negative breast cancer - eff Nov 13
https://www.fda.gov/drugs/drug-approvals-and-datab...
0 -
Lumpie you seem to be on a roll....thank you!
0 -
I did get on a bit of a roll. These were non-scientific but may affect access to care for many in the US, so thought I would share. Hope these help....
0 -
Existing antidepressant helps to inhibit growth of cancer cells in lab animals
New research has shown that the antidepressant sertraline helps to inhibit the growth of cancer cells...
Cancer cells use different biological mechanisms to stimulate their growth. In certain types of breast cancer, leukaemia, skin cancer, brain tumours and lung cancer, among others, the malignant cells produce large amounts of serine and glycine, two amino acids. This production stimulates the growth of cancer cells to such an extent that they become addicted to serine and glycine.
[A screening process involving 1600 yeast trials] showed that the antidepressant sertraline was the most effective substance. "Other studies had already indicated that sertraline has a certain anti-cancer activity, but there was no explanation for this yet", mention researchers Shauni Geeraerts (LDMC and CMPG) and Kim Kampen (LDMC). "In this study, we've been able to demonstrate that sertraline inhibits the production of serine and glycine, causing decreased growth of cancer cells. We also found that this substance is most effective in combination with other therapeutic agents. In studies with mice we saw that sertraline in combination with another therapy strongly inhibits the growth of breast cancer cells."
https://www.eurekalert.org/pub_releases/2020-11/kl...
0 -
I've been a baby aspirin taker for years since dx. I thought this article was interesting. Aspirin may be beneficial in patients who are not BRCA+ but harmful in BRCA + patients.
https://www.upi.com/Health_News/2019/08/12/Aspirin...
0 -
Another interesting post that someone made in another thread:
https://journals.lww.com/oncology-times/fulltext/2...
https://www.biorxiv.org/content/10.1101/2020.01.21...
Metformin may be helpful when metastasis is happening but harmful when BC cells are dormant and the patient is on and AI
0 -
One more interesting study - not breaking - but a small study to look at iodine either alone or in conjunction with chemo.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC66829...
0 -
Eating more fruits and vegetables may help breast cancer survivors live longer
We examined data on nearly 9,000 women with breast cancer who were followed for up to 30 years, and observed that those who consumed higher amounts of fruits and vegetables after their diagnosis were less likely to die during the study period than those with lower amounts of fruits and vegetables in their diets. High fruit and vegetable consumption, and high consumption of just vegetables, was associated with lower mortality from all causes—most women with breast cancer die from other causes. Some subgroups of fruits and vegetables were also associated with lower all-cause mortality, including leafy green vegetables, cruciferous vegetables such as broccoli, fruits and vegetables high in vitamin C, and vegetables high in beta-carotene.
We also observed that eating high amounts of blueberries was significantly associated with lower breast cancer-specific mortality, as well as all-cause mortality. This may be because blueberries contain bioactive components that may prevent or slow breast tumors from growing or spreading.
https://www.hsph.harvard.edu/news/features/breast-cancer-survival-fruits-vegetables/
0 -
Fertility Preservation Boosts Live Births after Breast Cancer
— Also associated with better survival
Fertility preservation (FP) appeared successful for women undergoing breast cancer treatment, data from a Swedish cohort showed.
About 23% of women who underwent FP had one or more live births after treatment for breast cancer, as compared with 9% of those going without it. FP was associated with 5- and 10-year cumulative incidences of post-breast cancer live births that were more than twice as high as rates for women who did not have FP.
https://www.medpagetoday.com/hematologyoncology/br...
Primary Source: JAMA Oncology
Source Reference: Marklund A, et al "Reproductive outcomes after breast cancer in women with vs without fertility preservation" JAMA Oncol 2020; DOI: 10.1001/jamaoncol.2020.5957.
{Free access to medical reporting. Sign-in may be required. Fee or subscripton will be required for full article access.}
0 -
repurposing drugs for triple negative breast cancer
https://www.researchgate.net/publication/342904316...
proton pump inhibitors like Prilosec look like they might be helpful along with chemo
very small study of 42 patients: https://meetinglibrary.asco.org/record/190369/abst...
0 -
pembrolizumab (Keytruda) for leptomeningeal mets - not just in triple neg breast pt. Pts in this study weren't even all breast ca pts
"Pembrolizumab (Keytruda) led to a 38% central nervous system (CNS) response rate and was well tolerated in patients with leptomeningeal metastasis (LMM) from solid tumors, according to phase 2 results" https://www.onclive.com/view/pembrolizumab-shows-i...
0 -
I'll be watching this one closely. There are currently no targeted treatments for p53 mutations and lots of cancers develop these mutations especially in late stage.
FDA Grants Fast Track to PC14586, Potential Therapy for Specific p53 Mutation
https://breastcancer-news.com/2020/10/29/fda-grant...
Here's the trial info. It's in San Antonio, TX.
https://clinicaltrials.gov/ct2/show/NCT04585750
0 -
techtonicshift
That is an interesting trial. I have genomic TP53 c.847C>T (Arg 283Cys) VUS. It is common in breast cancer but an “unknown significance” for now.
Dee
0 -
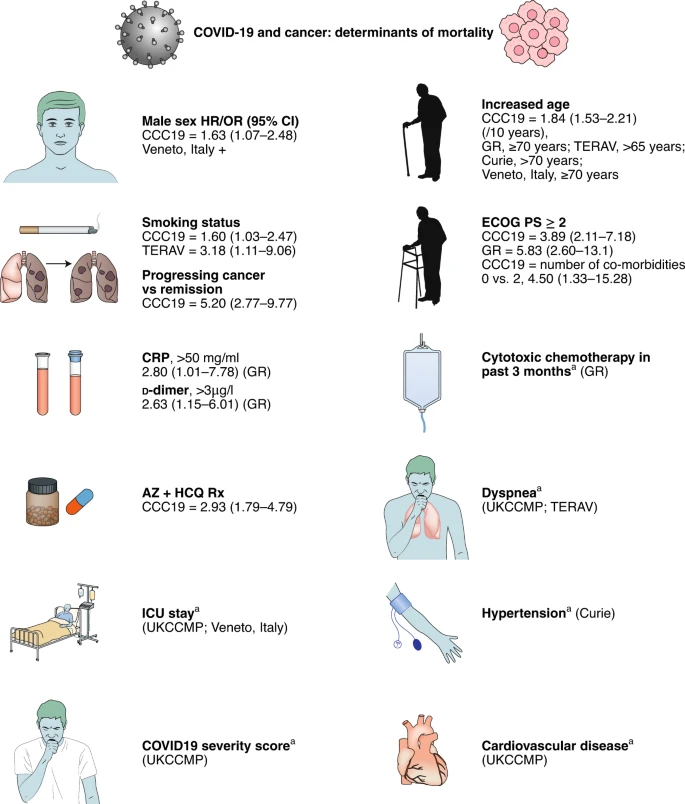
Covid & cancer - additional determinants of mortality
https://www.nature.com/articles/s43018-020-00129-w...
0 -
I am not sure if this is the place to post foods and supplements to avoid while in AI:
0 -
-
[CRISPR used to treat cancer in mice]
..."There are no side effects, and we believe that a cancer cell treated in this way will never become active again." Peer told the news outlet, adding, "This technology can extend the life expectancy of cancer patients and we hope, one day, cure the disease..."
The scientists used the technique on hundreds of mice – and Peer said the method could potentially be used on humans within two years.
The study focused on two types of cancers — glioblastoma, an aggressive type of cancer that can occur in the brain or spinal cord, and metastatic ovarian cancer.
Researchers found that mice with cancer who received the treatment had double the life expectancy of the control group, and their survival rate was 30 percent higher, the [Times of Israel] reported.
0 -
Thank you for sharing! CRISPR is so facinating. I would love to see more about this from a better news source than the NY Post! I do often look to CRISPR editing as the hope to end BRCA1 and BRCA2 mutations :-)
0 -
0
-
Interesting article from National Cancer Institute about treating bone mets with radiation
https://www.cancer.gov/news-events/cancer-currents...
0 -
Practicing Oncologists Debate New Tactics for Brain Metastases in HER2+ Breast Cancer
October 21, 2020OncologyLive
New approaches for treating patients with HER2-positive metastatic breast cancer are showing signs of efficacy against brain metastases, generating excitement about the potential to make critical advances and sparking questions about optimal sequencing.
Interview format article
https://www.onclive.com/view/practicing-oncologist...
{No charge for access but sign in may be required.}
0 -
-
NCI-MATCH Trial Identifies Actionable Alterations in More Than One-Third of Patients With Cancer
December 3, 2020
As part of the National Cancer Institute Molecular Analysis for Therapy Choice (NCI-MATCH) trial conducted at more 1000 study sites, researchers have identified actionable alterations in nearly 38% of patients with cancer, and almost 18% of patients were assigned to treatments based on their molecular profiling results.1 The patient population included a large proportion of patients with less common cancers, including gastroesophageal cancer, sarcoma, and kidney cancer, in addition to patients with the most common cancers — colorectal, breast, and prostate cancers, as well as non-small-cell lung carcinoma (NSCLC).
https://www.cancertherapyadvisor.com/home/cancer-t...
{Free access, registration may be required.}
0 -
Increased Overall Survival in Patients With MBC and Liver or Lung Metastases Treated With Eribulin
December 03, 2020
- In this retrospective study of 443 patients with metastatic breast cancer and liver or lung metastases who received third-line treatment with eribulin (n = 229), gemcitabine (n = 134), or capecitabine (n = 80), the authors evaluated overall survival in real-world clinical practice. A larger proportion of patients who received eribulin were alive at 6, 12, 24, and 36 months compared with those receiving gemcitabine, and more eribulin-treated patients were alive until 36 months compared with capecitabine-treated patients. Overall survival and survival among patients with TNBC and HR+/HER2− disease was numerically increased among patients who received eribulin.
- These real-world data support data from randomized clinical trials regarding the consistent effects of eribulin in this patient population.
{Free access}0 -
That’s very helpful Lumpie...I’m looking at what 3rd line treatment might look like for me, so this info gives me a chance to discuss with my MO. Good timing too as I speak with her this week!
0 -
Lumpie
I asked my MDACC team if I was in the match trial. They said yes, but never once contacted me about anything potential. I am learning that you have to be proactive to get on a trial and that sometimes it's all about timing.
My local MO read that erubulin paper. He said I can keep it in my bucket but he prefers me to try a platinum drug combo next because of the Neuroendocrine part.
Thanks for keeping us all informed!
Dee
0 -
I got this email from onclive -re. MBC if anyone wants to register for the webinar- Webinar for MBC
if the link doesn't work and you want to,you can LMK your email and I can forward the email to you?
0 -
Dee: Yes, it can seem kind of random getting on trials. Part of it is definitely timing. Other times it is all sorts of factors from timing to reaching the right person to the sheer luck of matching what is needed at any given moment. NIH tells me that they have a "desk" that is supposed to screen prospective participants for all of their breast cancer trials, but I have not felt like there was much clarity around how that screen/match process operated - you just have to trust it. I have sometimes thought .... it would be great if there were a central service that would screen and match you for all available clinical trials approved in the US. Seems to me like that might promote participation, fill trials more efficiently and allow for better management of patient participation. But I suppose that would be a sizable undertaking. Maybe someday.
0 -
re finding trials, I signed with Cancer Research Insititute and the service gave me a list of potential trials and there is an option for them to notify you if something new pops up. I doubt it will work well in Canada but I did it just to see. https://app.emergingmed.com/emed/home
0 -
I stumbled upon this article, and thought it was a very good (but sobering) article about the mechanisms of metastatic recurrence in breast cancer. This article covers the how, why, when, where, and what we can do about it.
I had my first metastatic recurrences this year. I went from NED after a local recurrence to innumerable metastatic lesions in only a few months. That blindsided me, and hit me like a freight train. In these situations it sometimes helps me to understand the science and the mechanisms behind why and how these things happen. I thought this article might be helpful for others, too.
Here are a few key takeaways from the conclusions sections, but the whole article is really interesting:
"[O]ur current understanding of metastatic dormancy, metastatic evolution, acquired resistance and metastatic niches suggests that detecting and treating recurrence earlier might be our best opportunity to improve patient outcomes.
Despite metastatic disease being the main cause of death in cancer patients, knowledge about the biology of this lethal process is lacking. However, with advances in genomic sequencing technologies and accumulating data in favour of the predominance of the parallel model over the linear model of dissemination, four important lessons have been learned. First, in most patients who will experience recurrence, metastases are already present at the time of diagnosis. Second, despite their genomic similarity to the trunk of the tumour's evolutionary tree, metastases are distinct biological entities, containing important phenotypic differences compared with their primary source. Third, metastases, as well as primary neoplasms, are subject to evolution dictated by pharmacological pressure, tissue-specific environments and cellular plasticity. Finally, some micrometastases might exist in a non-proliferative, dormant-like state for months to decades.
Altogether, these data have significant clinical implications. First, attempts to prevent initial metastatic dissemination might hold little therapeutic benefit—even though early detection and treatment of most primary breast tumours is curative, tumours that are 'born to be bad' probably disseminate prior to diagnosis. Next, caution must be taken when using primary tumours as a proxy for clinical decisions on systemic therapies to prevent or treat metastatic disease, unless little divergence between paired lesions is observed. In this respect, non-invasive liquid biopsy biomarker assays could help to identify molecular changes in metastases. In addition, an urgent need exists to assess the phenotypic properties of DTCs in their native states, in order to understand how some DTCs, but not others, contribute to metastatic recurrence. Finally, it might be possible to exploit tumour dormancy in some, but probably not all, cases as a window of opportunity to tackle MRD and/or prevent metastatic relapse (Table 1).
Future directions should be centred on identifying dangerous versus indolent DTCs and finding new DTC drug targets, while also using modern imaging and biomarker assays to accurately determine who needs such therapy, in order to avoid overtreatment. Importantly, all of the above strategies—prevent, reverse, prolong and eradicate dormancy (Table 1)—will require the development and use of more clinically relevant models and human samples, as well as clinical trials of new 'intensive' follow-up monitoring programmes. With progress in these areas, it is hoped that new knowledge will converge in the near future to prevent recurrences and deaths from cancer."
0